

Amyloid-β oligomerization in Alzheimer dementia versus high-pathology controls
- PMID: 23225543
- PMCID: PMC3563737
- DOI: 10.1002/ana.23748
Amyloid-β oligomerization in Alzheimer dementia versus high-pathology controls
Abstract
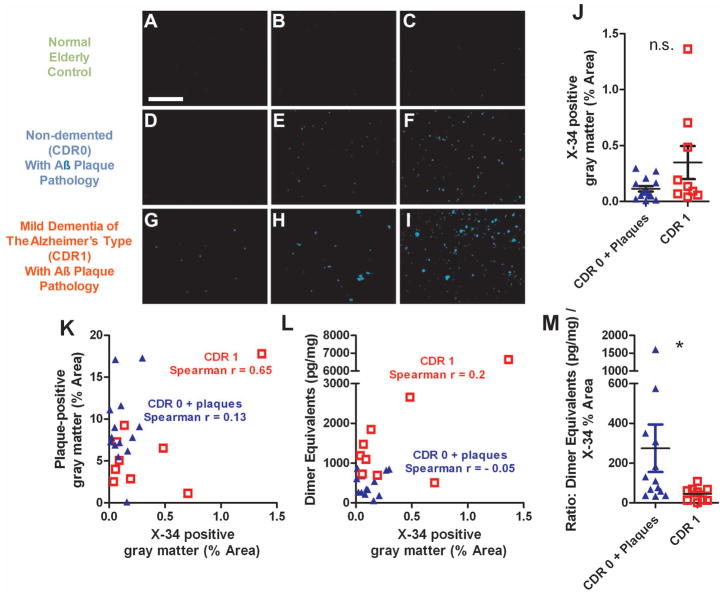
Objective: Although amyloid-beta (Aβ) peptide deposition into insoluble plaques is a pathological hallmark of Alzheimer disease; soluble oligomeric Aβ has been hypothesized to more directly underlie impaired learning and memory in dementia of the Alzheimer type. However, the lack of a sensitive, specific, and quantitative assay for Aβ oligomers has hampered rigorous tests of this hypothesis.
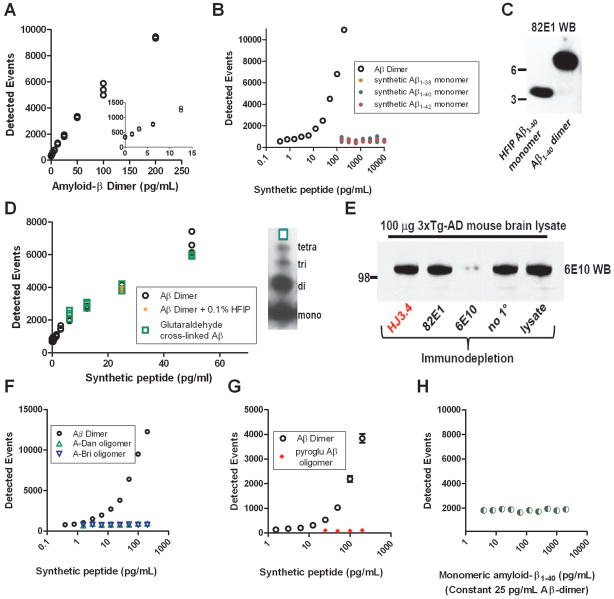
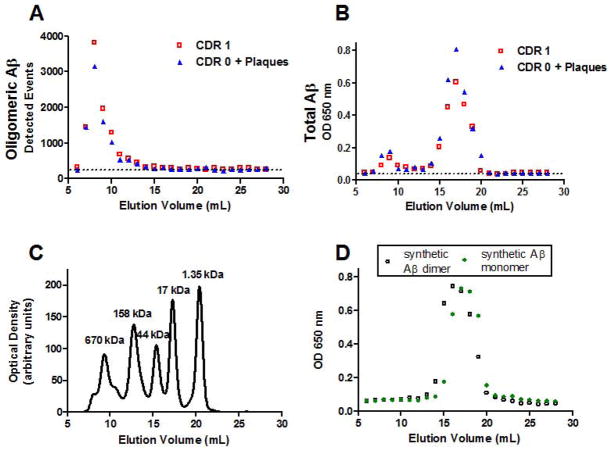
Methods: We developed a plate-based single molecule counting fluorescence immunoassay for oligomeric Aβ sensitive to low pg/ml concentrations of synthetic Aβ dimers using the same Aβ-specific monoclonal antibody to both capture and detect Aβ. The Aβ oligomer assay does not recognize monomeric Aβ, amyloid precursor protein, or other non-Aβ peptide oligomers.
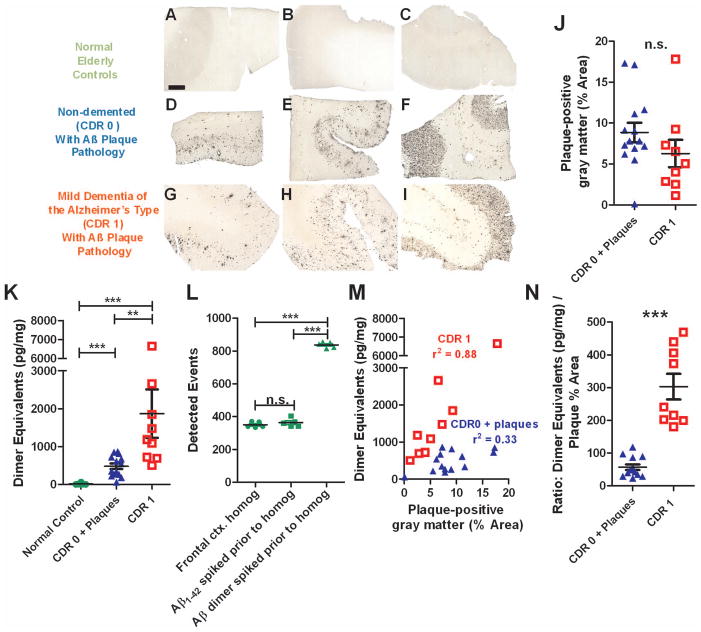
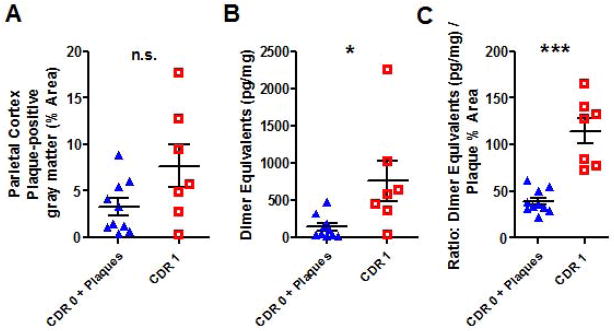
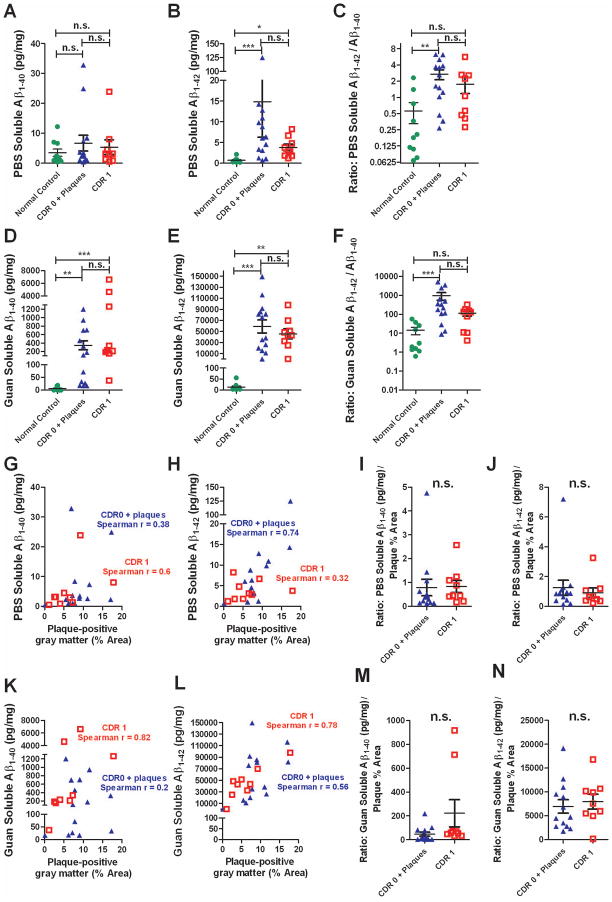
Results: Aβ oligomers were detected in aqueous cortical lysates from patients with dementia of the Alzheimer type and nondemented patients with Aβ plaque pathology. However, Aβ oligomer concentrations in demented patients' lysates were tightly correlated with Aβ plaque coverage (r = 0.88), but this relationship was weaker in those from nondemented patients (r = 0.30) despite equivalent Aβ plaque pathology. The ratio of Aβ oligomer levels to plaque density fully distinguished demented from nondemented patients, with no overlap between groups in this derived variable. Other Aβ and plaque measures did not distinguish demented from nondemented patients. Aβ oligomers were not detected in cerebrospinal fluid with this assay.
Interpretation: The results raise the intriguing hypothesis that the linkage between plaques and oligomers may be a key pathophysiological event underlying dementia of the Alzheimer type. This Aβ oligomer assay may be useful for many tests of the oligomer hypothesis.
Copyright © 2012 American Neurological Association.
Figures
References
-
- Price JL, Morris JC. Tangles and plaques in nondemented aging and “preclinical” Alzheimer’s disease. Annals of neurology. 1999 Mar;45(3):358–68. - PubMed
-
- Hulette CM, Welsh-Bohmer KA, Murray MG, Saunders AM, Mash DC, McIntyre LM. Neuropathological and neuropsychological changes in “normal” aging: evidence for preclinical Alzheimer disease in cognitively normal individuals. Journal of neuropathology and experimental neurology. 1998 Dec;57(12):1168–74. - PubMed
-
- Katzman R, Terry R, DeTeresa R, et al. Clinical, pathological, and neurochemical changes in dementia: a subgroup with preserved mental status and numerous neocortical plaques. Annals of neurology. 1988 Feb;23(2):138–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R-01-NS065667/NS/NINDS NIH HHS/United States
- R01 AG013956/AG/NIA NIH HHS/United States
- R01 NS065667/NS/NINDS NIH HHS/United States
- P50 AG005681/AG/NIA NIH HHS/United States
- AG13956/AG/NIA NIH HHS/United States
- K-23-AG030946/AG/NIA NIH HHS/United States
- R37 AG013956/AG/NIA NIH HHS/United States
- K08 NS049237/NS/NINDS NIH HHS/United States
- P50-AG05681/AG/NIA NIH HHS/United States
- AG029524/AG/NIA NIH HHS/United States
- R01 NS065069/NS/NINDS NIH HHS/United States
- P01-AG03991/AG/NIA NIH HHS/United States
- P30 NS057105/NS/NINDS NIH HHS/United States
- K01 AG029524/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
