

Patient characteristics, treatment patterns, and health outcomes among COPD phenotypes
- PMID: 23226014
- PMCID: PMC3514008
- DOI: 10.2147/COPD.S35501
Patient characteristics, treatment patterns, and health outcomes among COPD phenotypes
Abstract
Background: Recent literature has suggested that emphysema and chronic bronchitis, traditionally considered to be entities overlapping within chronic obstructive pulmonary disease (COPD), may be distinct disorders. Few studies have examined the differences in patient characteristics and health outcomes between these conditions. This study examined whether COPD phenotypes represent distinct patient populations, in a large nationally representative US sample.
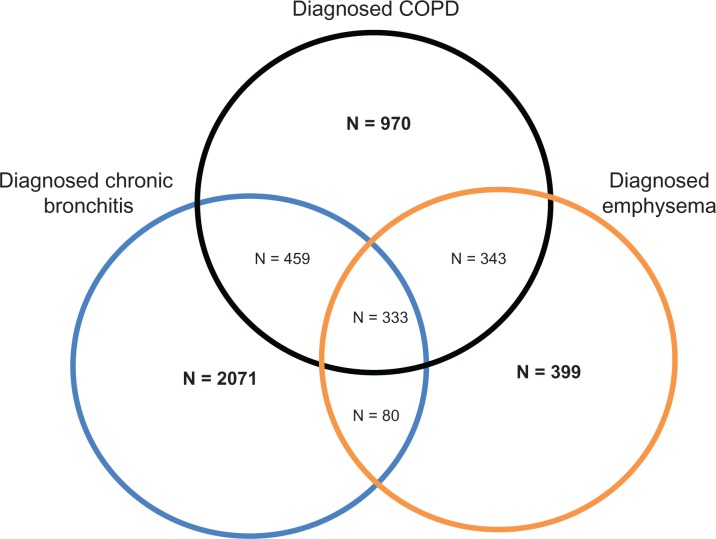
Methods: Data were obtained from the 2010 US National Health and Wellness Survey (NHWS). NHWS respondents (n = 75,000) were categorized as a COPD phenotype based on their self-reported diagnosis of COPD only (n = 970), emphysema only (n = 399), or chronic bronchitis only (n = 2071). Phenotypes were compared on demographics, health characteristics, treatment patterns, health outcomes, work productivity, and resource use. Variables were compared using Chi-square and analysis of variance tests for categorical and continuous outcomes, respectively. Health outcomes were also examined using regression modeling, controlling for demographic and health characteristic covariates.
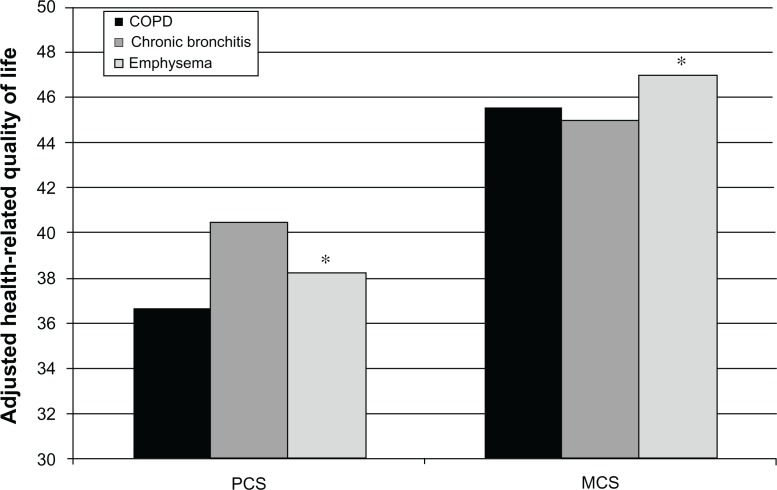
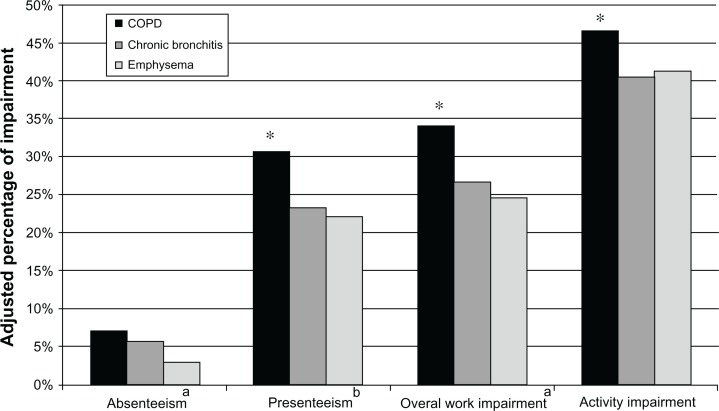
Results: Patients with chronic bronchitis were significantly younger (51.38 years versus 63.24 years for COPD versus 63.30 years for emphysema, P < 0.05) and more likely to be employed (46.98% versus 23.81% for COPD versus 28.33% for emphysema, P < 0.05). Relative to the other phenotypes, patients with chronic bronchitis were also significantly more likely to be female, nonwhite, and to exercise currently (all P < 0.05), and were significantly less likely to be a current or former smoker (P < 0.05). Controlling for demographic and health characteristics, patients self-identified as having COPD only reported significantly worse physical quality of life (adjusted mean 36.69) and health utilities (adjusted mean 0.65) and significantly more absenteeism (adjusted mean 7.08%), presenteeism (adjusted mean 30.73%), overall work impairment (adjusted mean 34.06%), and activity impairment (adjusted mean 46.59%) than the other phenotypes (all P < 0.05).
Conclusion: These results suggest considerable heterogeneity among different COPD phenotypes with respect to demographics, health characteristics, disease characteristics, treatment patterns, and health outcomes. Research aimed at understanding the differences in patient characteristics and disease presentation of these phenotypes could be used to guide treatment recommendations.
Keywords: chronic bronchitis; chronic obstructive pulmonary disease; emphysema; health care resource use; quality of life; work productivity.
Figures
References
-
- Mannino DM. Chronic obstructive pulmonary disease: epidemiology and evaluation. Hosp Physician. 2001;37(10):22–31.
-
- Soriano JB, Davis KJ, Coleman B, Visick G, Mannino D, Pride NB. The proportional Venn diagram of obstructive lung disease: two approximations from the United States and the United Kingdom. Chest. 2003;124(2):474–481. - PubMed
-
- Agusti A, Vestbo J. Current controversies and future perspectives in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;184(5):507–513. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
