

The future role of personalized medicine in the treatment of glioblastoma multiforme
- PMID: 23226047
- PMCID: PMC3513213
- DOI: 10.2147/PGPM.S6852
The future role of personalized medicine in the treatment of glioblastoma multiforme
Abstract
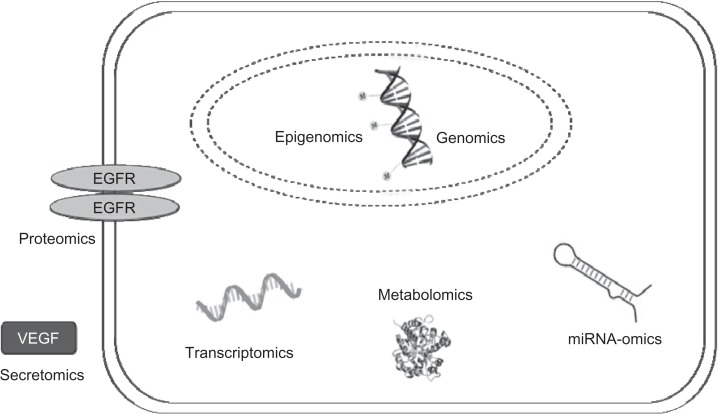
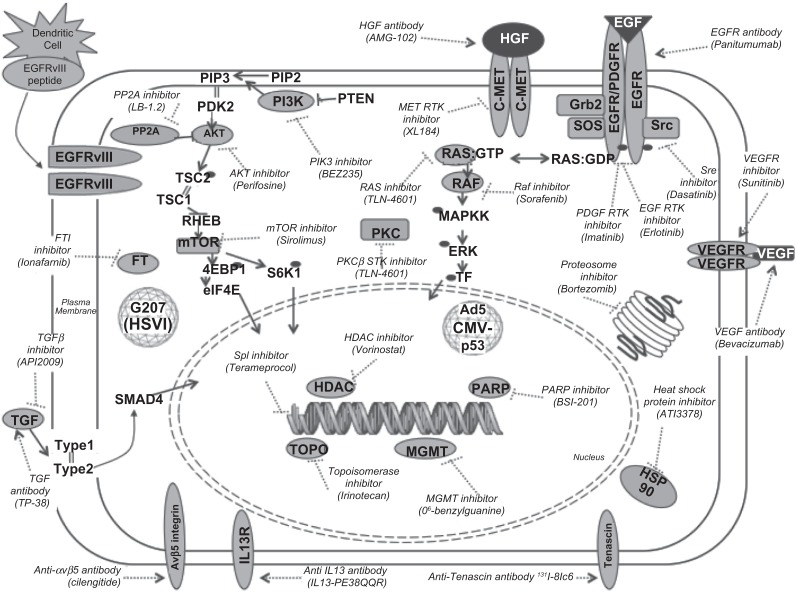
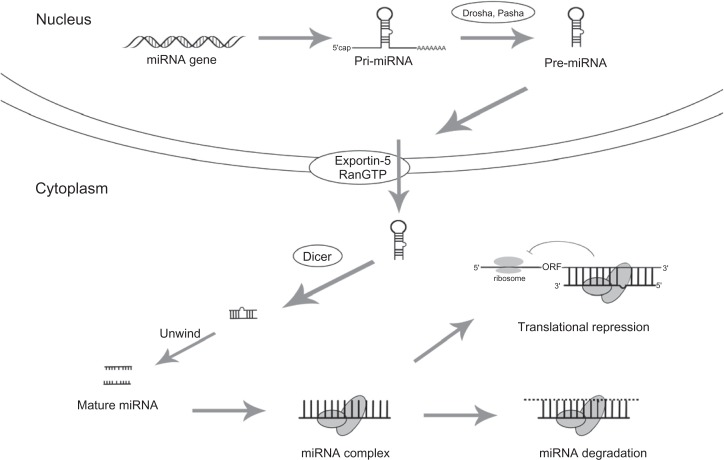
Glioblastoma multiforme (GBM) remains one of the most malignant primary central nervous system tumors. Personalized therapeutic approaches have not become standard of care for GBM, but science is fast approaching this goal. GBM's heterogeneous genomic landscape and resistance to radiotherapy and chemotherapy make this tumor one of the most challenging to treat. Recent advances in genome-wide studies and genetic profiling show that there is unlikely to be a single genetic or cellular event that can be effectively targeted in all patients. Instead, future therapies will likely require personalization for each patient's tumor genotype or proteomic profile. Over the past year, many investigations specifically focused simultaneously on strategies to target oncogenic pathways, angiogenesis, tumor immunology, epigenomic events, glioma stem cells (GSCs), and the highly migratory glioma cell population. Combination therapy targeting multiple pathways is becoming a fast growing area of research, and many studies put special attention on small molecule inhibitors. Because GBM is a highly vascular tumor, therapy that directs monoclonal antibodies or small molecule tyrosine kinase inhibitors toward angiogenic factors is also an area of focus for the development of new therapies. Passive, active, and adoptive immunotherapies have been explored by many studies recently, and epigenetic regulation of gene expression with microRNAs is also becoming an important area of study. GSCs can be useful targets to stop tumor recurrence and proliferation, and recent research has found key molecules that regulate GBM cell migration that can be targeted by therapy. Current standard of care for GBM remains nonspecific; however, pharmacogenomic studies are underway to pave the way for patient-specific therapies that are based on the unique aberrant pathways in individual patients. In conclusion, recent studies in GBM have found many diverse molecular targets possible for therapy. The next obstacle in treating this fatal tumor is ascertaining which molecules in each patient should be targeted and how best to target them, so that we can move our current nonspecific therapies toward the realm of personalized medicine.
Keywords: GBM; genetics; oncogenomics; pharmacogenomics; signaling cascades.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Sehati N, Liau L. Adjuvant treatment for gliomas. Contemp Neurosurg. 2003;25(15):1–10.
-
- Central Brain Tumor Registry of the United States . Statistical report: primary brain tumors in the United States, 2000–2004. Chicago: Central Brain Tumor Registry of the United States; 2008.
-
- Ohgaki H, Dessen P, Jourde B, et al. Genetic pathways to glioblastoma: a population-based study. Cancer Res. 2004;64(19):6892–6899. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
