

Utility of cardiac magnetic resonance in the evaluation of unselected patients with possible arrhythmogenic right ventricular cardiomyopathy
- PMID: 23226076
- PMCID: PMC3511051
- DOI: 10.4137/CMC.S9996
Utility of cardiac magnetic resonance in the evaluation of unselected patients with possible arrhythmogenic right ventricular cardiomyopathy
Abstract
Introduction: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a rare but important cause of sudden cardiac death. We investigated the role of cardiac magnetic resonance imaging (CMR) in the evaluation of patients with suspected ARVC referred by a general cardiology service.
Methods: Ninety-two patients (mean age 48 ± 15, 49% female), referred for CMR assessment of possible ARVC, were reviewed. CMR included both functional and tissue characteristic imaging.
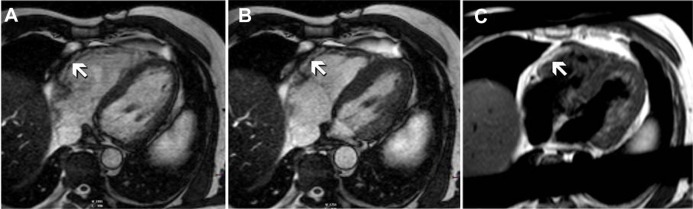
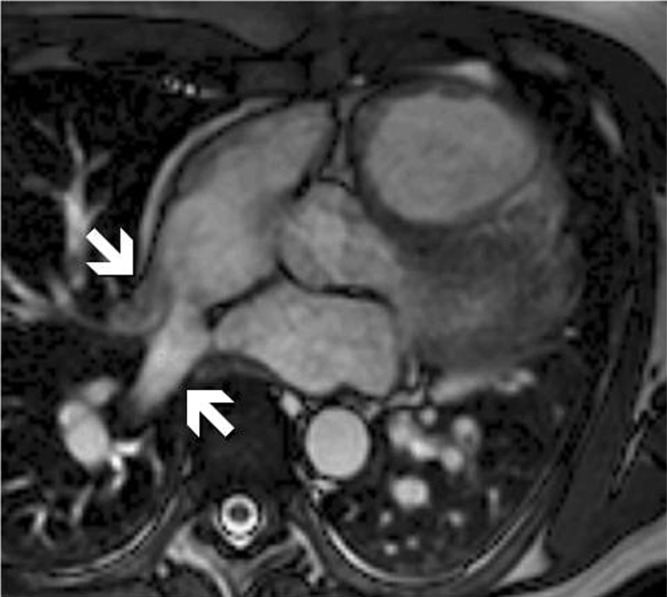
Results: No patients had ARVC based on the 1994 Task Force Criteria (TFC) prior to CMR, but 4 met proposed Modified TFC; 15% met one major (±1 minor) TFC, 71% 1 or 2 minor TFC, and 14% no TFC. Reasons for CMR referral included symptomatic arrhythmia of likely RV origin (28%), Electrocardiogram/Holter abnormalities (28%), echocardiographic features suspicious of ARVC (19%), and family history of ARVC (8%). CMR findings strongly suggestive of ARVC were found in nine patients (10%), although only three were considered typical. Of these patients two met 1 major TFC and seven met 1 or 2 minor TFC. CMR findings included RV thinning, aneurysm, and diastolic out-pouching, but only 1 patient had definite fatty infiltration of the RV. Incidentally, CMR detected important, previously undiagnosed pathology, including anomalous pulmonary venous drainage (2 patients) and non-ischaemic cardiomyopathy (6%). CMR was normal in 63%, with minor abnormalities in 29%.
Conclusions: CMR may play an important diagnostic role in the evaluation of possible ARVC. Patients who do not meet TFC for diagnosis may have CMR features typical of ARVC. Additionally CMR may detect other hitherto undiagnosed structural or functional abnormalities that alter patient management. However the majority of patients referred have a low pretest probability of ARVC, and the rate of normal CMR scans is high.
Keywords: cardiac magnetic resonance imaging; cardiomyopathy.
Figures
References
-
- Marcus F, Fontaine G, Guiraudon G, et al. Right ventricular dysplasia: a report of 24 adult cases. Circulation. 1982;65:384–98. - PubMed
-
- Sen-Chowdhry S, Lowe MD, Sporton SC, McKenna WJ. Arrhythmogenic right ventricular cardiomyopathy: Clinical presentation, diagnosis, and management. Am J Med. 2004 Nov 1;117(9):685–95. - PubMed
-
- Angelini A, Basso C, Nava A, Thiene G. Endomyocardial biopsy in arrhythmogenic right ventricular cardiomyopathy. Am Heart J. 1996 Jul;132(1 Pt 1):203–6. - PubMed
-
- McKenna WJ, Thiene G, Nava A, et al. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Br Heart J. 1994 Mar;71(3):215–8. - PMC - PubMed
-
- Hamid MS, Norman M, Quraishi A, et al. Prospective evaluation of relatives for familial arrhythmogenic right ventricular cardiomyopathy/dysplasia reveals a need to broaden diagnostic criteria. J Am Coll Cardiol. 2002 Oct 16;40(8):1445–50. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
