

Clinical analysis and misdiagnosis of cerebral venous thrombosis
- PMID: 23226750
- PMCID: PMC3493792
- DOI: 10.3892/etm.2012.697
Clinical analysis and misdiagnosis of cerebral venous thrombosis
Abstract
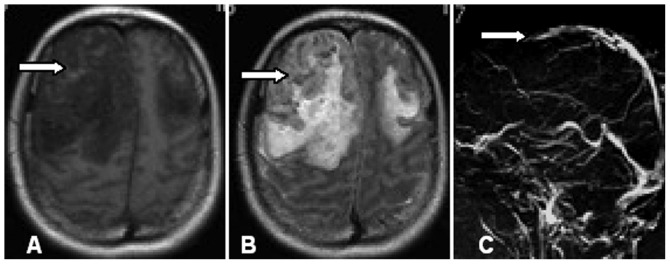
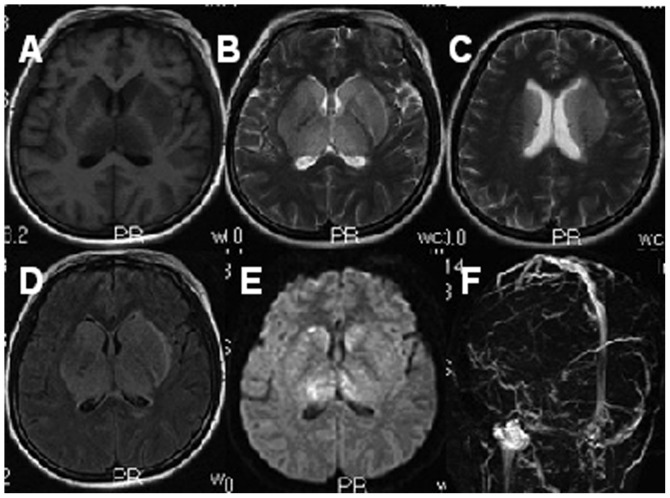
The present study aimed to summarize the clinical characteristics and experiences of misdiagnoses of cerebral venous thrombosis (CVT). A total of 18 patients with CVT who received treatment between September 2009 and August 2011 were enrolled. Of the patients, 13 were females and 5 were males with an average age of 39 years. Clinical manifestations and characteristics according to cerebrospinal fluid examination and imaging were summarized retrospectively. CVT principally manifested as headaches, papilledema, psychiatric symptoms, impaired consciousness and seizure disorders, with or without neurological defects. A combination of magnetic resonance imaging (MRI) and venography (MRV) was demonstrated to be an effective method for CVT diagnosis. Of the 18 patients, 8 were misdiagnosed, as a result of the lack of further examination due to undefined etiology, atypical clinical manifestations and ambiguous neuroimaging direct signs. The clinical symptoms of CVT are aspecific, as a result of which misdiagnosis tends to occur. For patients with intracranial hypertension accompanied with or without neurological defects, MRI combined with MRV can improve the accuracy of CVT diagnosis.
Figures
References
-
- Santos GR, André R, Pereira SL, Parreira T, Machado E. Cerebral venous thrombosis: retrospective analysis of 49 cases. Acta Med Port. 2011;24:21–28. (in Portuguese). - PubMed
-
- Poon CS, Chang JK, Swarnkar A, Johnson MH, Wasenko J. Radiologic diagnosis of cerebral venous thrombosis: pictorial review. AJR Am J Roentgenol. 2007;189:S64–S75. - PubMed
-
- Crombé D, Haven F, Gille M. Isolated deep cerebral venous thrombosis diagnosed on CT and MR imaging. A case study and literature review. JBR-BTR. 2003;86:257–261. - PubMed
-
- Rodallec MH, Krainik A, Feydy A, et al. Cerebral venous thrombosis and multidetector CT angiography: tips and tricks. Radiographics. 2006;26:S5–S18. - PubMed
LinkOut - more resources
Full Text Sources