

Differences in the acute effects of aerobic and resistance exercise in subjects with type 2 diabetes: results from the RAED2 Randomized Trial
- PMID: 23227155
- PMCID: PMC3515569
- DOI: 10.1371/journal.pone.0049937
Differences in the acute effects of aerobic and resistance exercise in subjects with type 2 diabetes: results from the RAED2 Randomized Trial
Abstract
Objective: Both aerobic (AER) and resistance (RES) training, if maintained over a period of several months, reduce HbA1c levels in type 2 diabetes subjects. However, it is still unknown whether the short-term effects of these types of exercise on blood glucose are similar. Our objective was to assess whether there may be a difference in acute blood glucose changes after a single bout of AER or RES exercise.
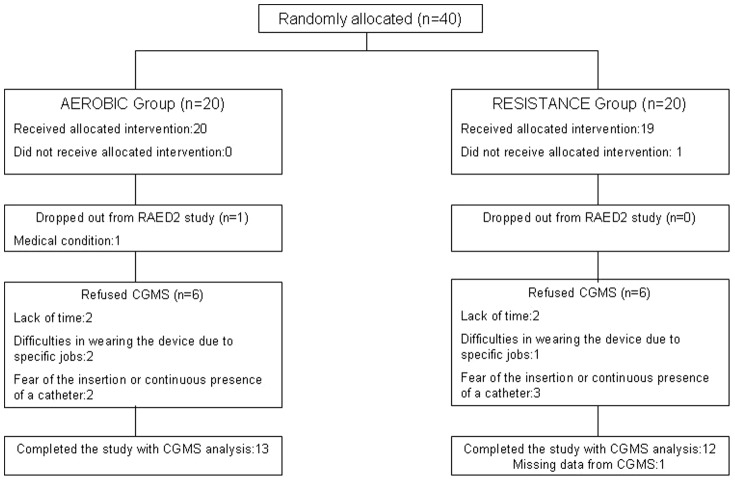
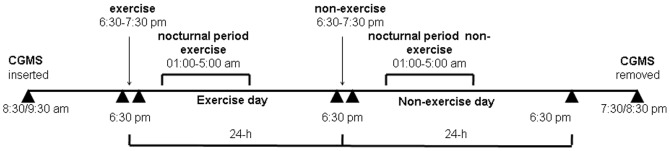
Study design: Twenty-five patients participating in the RAED2 Study, a RCT comparing AER and RES training in diabetic subjects, were submitted to continuous glucose monitoring during a 60-min exercise session and over the following 47 h. These measurements were performed after 10.9+0.4 weeks of training. Glucose concentration areas under the curve (AUC) during exercise, the subsequent night, and the 24-h period following exercise, as well as the corresponding periods of the non-exercise day, were assessed. Moreover, the low (LBGI) and high (HBGI) blood glucose indices, which summarize the duration and extent of hypoglycaemia or hyperglycaemia, respectively, were measured.
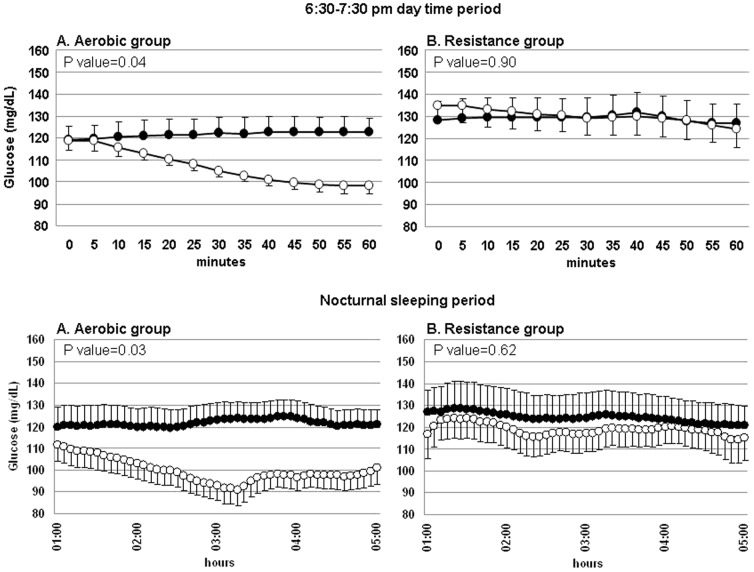
Results: AER and RES training similarly reduced HbA1c. Forty-eight hour glucose AUC was similar in both groups. However, a comparison of glucose AUC during the 60-min exercise period and the corresponding period of the non-exercise day showed that glucose levels were lower during exercise in the AER but not in the RES group (time-by-group interaction p = 0.04). Similar differences were observed in the nocturnal periods (time-by-group interaction p = 0.02). Accordingly, nocturnal LBGI was higher in the exercise day than in the non-exercise day in the AER (p = 0.012) but not in the RES group (p = 0.62).
Conclusions: Although AER and RES training have similar long-term metabolic effects in diabetic subjects, the acute effects of single bouts of these exercise types differ, with a potential increase in late-onset hypoglycaemia risk after AER exercise.
Trial registration: ClinicalTrials.gov NCT01182948.
Conflict of interest statement
Figures
References
-
- Sigal RJ, Kenny GP, Boulé NG, Wells GA, Prud'homme D, et al. (2007) Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: a randomized trial. Ann Intern Med 147: 357–69. - PubMed
-
- Suh SH, Paik IY, Jacobs K (2007) Regulation of blood glucose homeostasis during prolonged exercise. Mol Cells 23: 272–279. - PubMed
