

Trends in asthma-related direct medical costs from 2002 to 2007 in British Columbia, Canada: a population based-cohort study
- PMID: 23227222
- PMCID: PMC3515523
- DOI: 10.1371/journal.pone.0050949
Trends in asthma-related direct medical costs from 2002 to 2007 in British Columbia, Canada: a population based-cohort study
Erratum in
- PLoS One. 2013;8(6). doi:10.1371/annotation/a3275f00-6d75-4430-a0d6-5b4397ba501a
Abstract
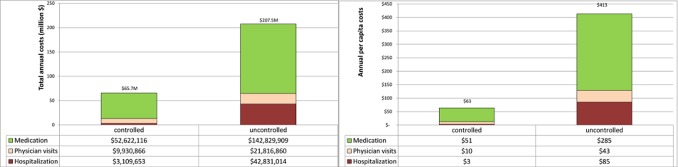
Background: Asthma-related health resource use and costs may be influenced by increasing asthma prevalence, changes to asthma management guidelines, and new medications over the last decade. The objective of this work was to analyze direct asthma-related medical costs, and trends in total and per-patient costs of hospitalizations, physician visits, and medications.
Methods: A cohort of asthma patients from British Columbia (BC), Canada, was created. Asthma patients were identified using a validated case definition. Costs for hospitalizations, physician visits, and medications were calculated from billing records (in 2008 Canadian dollars). Trends in total and per-patient costs over the study period were analyzed using Generalized Linear Models.
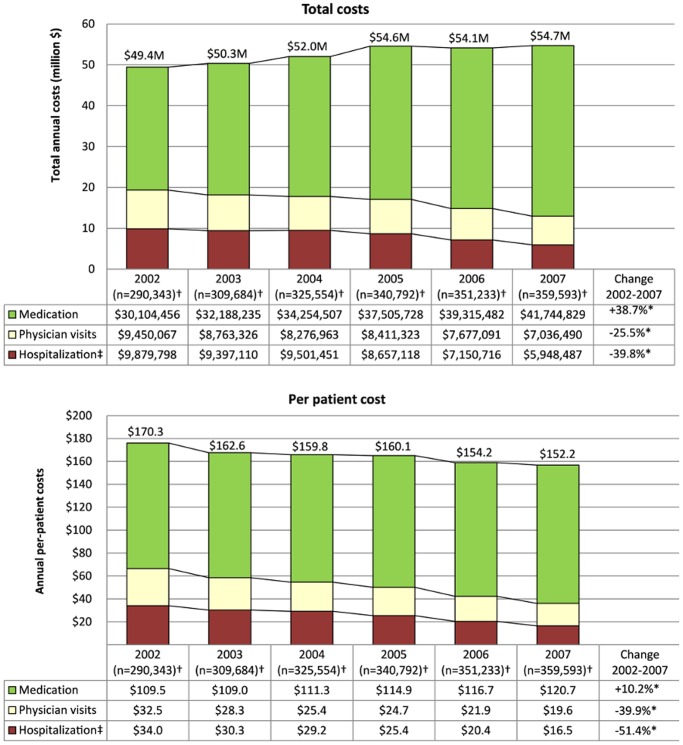
Results: 398,235 patients satisfied the asthma case definition (mid-point prevalence 8.0%). Patients consumed $315.9 million (M) in direct asthma-related health resources between 2002 and 2007. Hospitalizations, physician visits, and medication costs accounted for 16.0%, 15.7% and 68.2% of total costs, respectively. Cost of asthma increased from $49.4 M in 2002 to $54.7 M in 2007. Total annual costs attributable to hospitalizations and physician visits decreased (-39.8% and -25.5%, respectively; p<0.001), while medication costs increased (+38.7%; p<0.001).
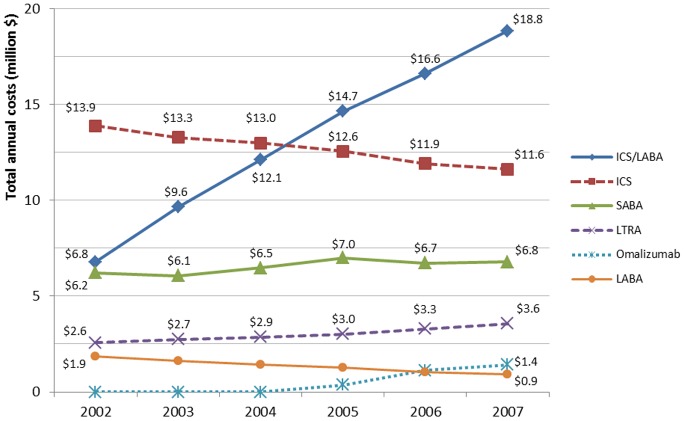
Interpretation: This population-based analysis shows that the total direct cost of asthma in BC has increased since 2002, mainly due to a rise in asthma prevalence and cost of medication. Combination therapy with inhaled corticosteroids/long-acting beta-agonists has become a significant component of the cost of asthma. Although billing records capture only a fraction of the true burden of asthma, the simultaneous increase in medication costs and reductions in hospitalization and physician visit costs provides valuable insight for policy makers into the shifts in asthma-related resource use.
Conflict of interest statement
Figures
References
-
- Masoli M, Fabian D, Holt S, Beasley R (2004) The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy 59: 469–478 doi:10.1111/j.1398–9995.2004.00526.x [doi] ALL526 [pii] - DOI - PubMed
-
- Braman SS (2006) The global burden of asthma. Chest 130: 4S–12S doi:10.1378/chest.130.1_suppl.4S - DOI - PubMed
-
- Gershon AS, Guan J, Wang C, To T (2010) Trends in asthma prevalence and incidence in Ontario, Canada, 1996–2005: a population study. Am J Epidemiol 172: 728–736 doi:10.1093/aje/kwq189 - DOI - PubMed
-
- Aaron SD, Vandemheen KL, Boulet L-P, McIvor RA, Fitzgerald JM, et al. (2008) Overdiagnosis of asthma in obese and nonobese adults. CMAJ 179: 1121–1131 doi:10.1503/cmaj.081332 - DOI - PMC - PubMed
-
- Bahadori K, Doyle-Waters MM, Marra C, Lynd L, Alasaly K, et al. (2009) Economic burden of asthma: a systematic review. BMC Pulm Med 9: 24 doi:10.1186/1471-2466-9-24 - DOI - PMC - PubMed
