

French "real life" experience of clofarabine in children with refractory or relapsed acute lymphoblastic leukaemia
- PMID: 23227903
- PMCID: PMC3599405
- DOI: 10.1186/2162-3619-1-39
French "real life" experience of clofarabine in children with refractory or relapsed acute lymphoblastic leukaemia
Abstract
Background: Clofarabine alone or in combination with cyclophosphamide and etoposide has shown a good efficacy and a tolerable toxicity profile in previous studies of children with relapsed or refractory leukaemia. This report describes a retrospective study of 38 French patients who received clofarabine as a monotherapy or in combination for relapsed or refractory acute lymphoblastic leukaemia (ALL) outside of clinical trials after marketing authorization.
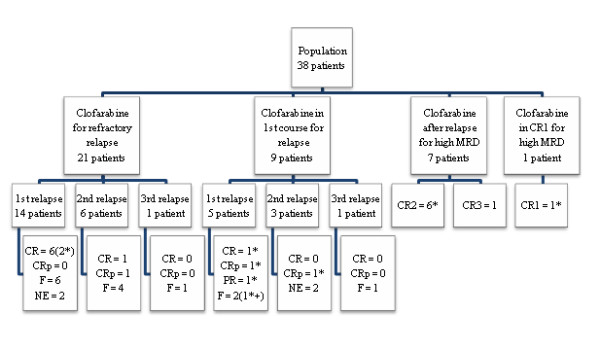
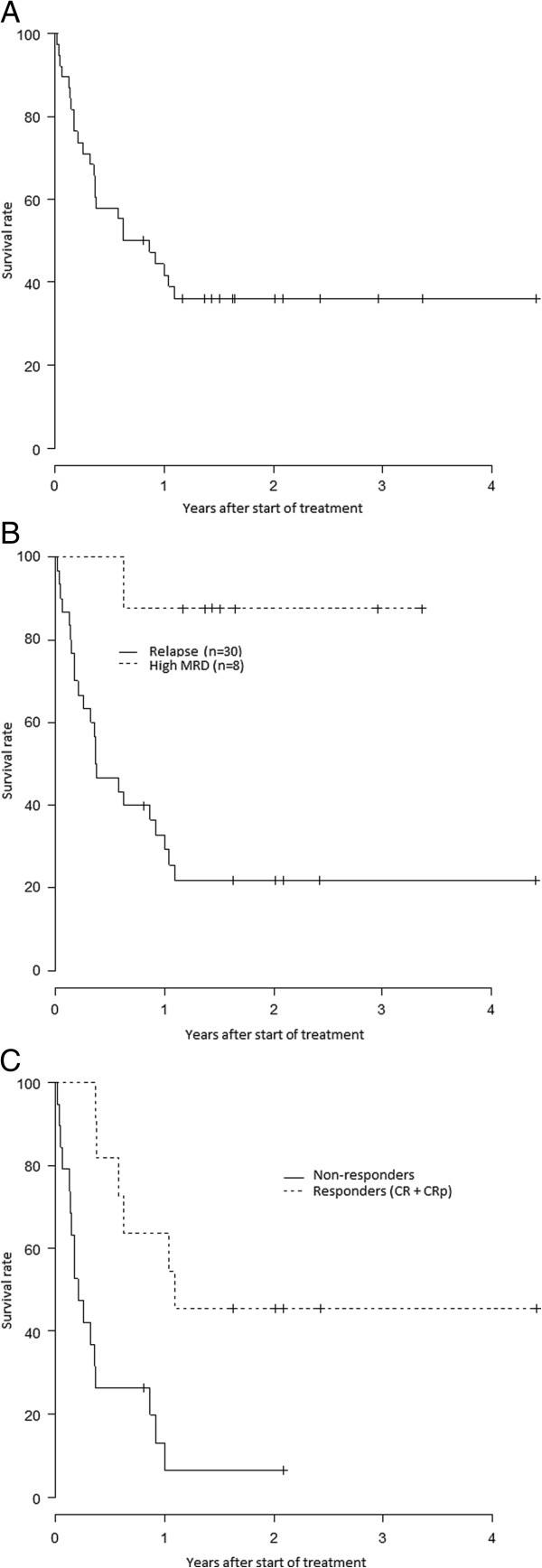
Methods: We retrospectively analysed data for 38 patients, up to 21 years old, attending 17 French centres. Thirty patients received clofarabine alone or in combination for a bone marrow relapse of acute lymphoblastic leukaemia (ALL) or refractory disease and eight patients for a high level of minimal residual disease (MRD). Survival and response durations were estimated by the Kaplan-Meier method.
Results: For the 30 patients who received clofarabine for a bone marrow relapse of ALL (number of relapse, 1-3; median, 1), the overall remission rate (ORR) was 37%: eight complete remission (CR) and three complete remission without platelet recovery (CRp). Ten of the 11 responding patients subsequently underwent haematopoietic stem cell transplantation (HSCT).Only four of the eight patients who received clofarabine while in remission for a high level of MRD, showed a moderate improvement of MRD. Seven of these eight patients received HSCT and six of them were alive at the end of the study. One other patient was alive without receiving HSCT.However, clofarabine treatment was associated with a high risk of infection and hepatotoxicity. Febrile neutropenia grade ≥ 3 was reported in 79% of patients and documented infections grade ≥ 3 occurred in nine patients (24%). Hepatotoxicity grade 3 was reported in nine patients (24%). We observed four deaths related to treatment.
Conclusion: In our experience, the efficacy of clofarabine is poorer than previously reported. Its toxicity is high and can be life threatening. Prospective studies on clofarabine used during earlier phases of the disease may help to define how best this new drug can be exploited for childhood and adolescent ALL.
Figures

References
-
- Raetz EA, Borowitz MJ, Devidas M, Linda SB, Hunger SP, Winick NJ, Camitta BM, Gaynon PS, Carroll WL. Reinduction platform for children with first marrow relapse of acute lymphoblastic leukemia: a children’s oncology group study. J Clin Oncol. 2008;26:3971–3978. doi: 10.1200/JCO.2008.16.1414. - DOI - PMC - PubMed
-
- Malempati S, Gaynon PS, Sather H, La MK, Stork LC. Outcome after relapse among children with standard-risk acute lymphoblastic leukemia: children’s oncology group study CCG-1952. J Clin Oncol. 2007;36:5800–5807. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
