

Devices in the management of advanced, chronic heart failure
- PMID: 23229137
- PMCID: PMC3753073
- DOI: 10.1038/nrcardio.2012.178
Devices in the management of advanced, chronic heart failure
Abstract
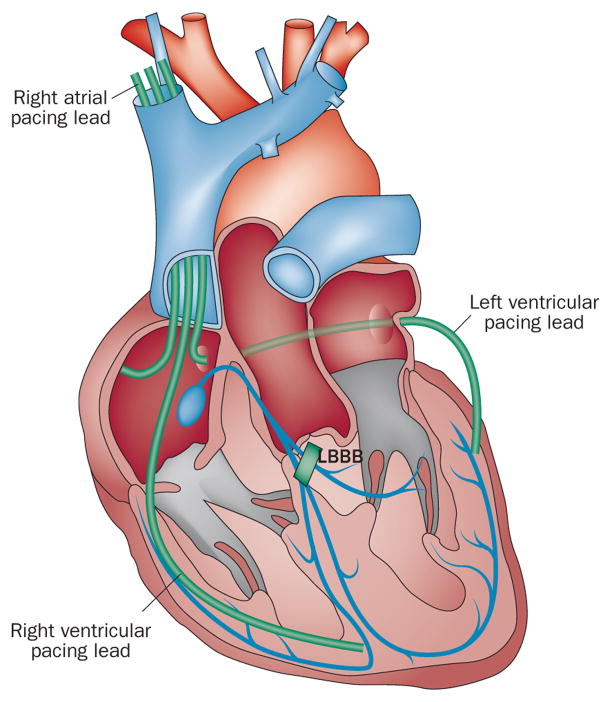
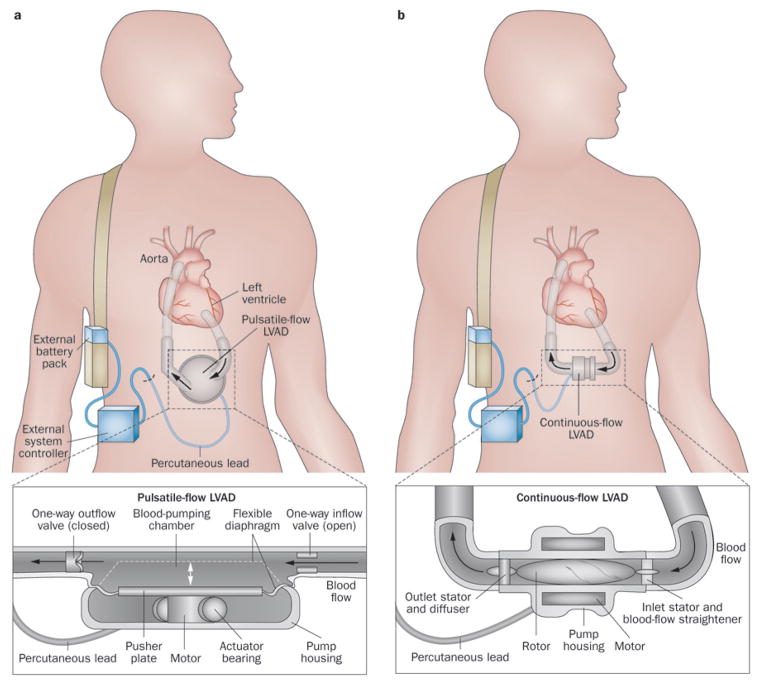
Heart failure (HF) is a global phenomenon, and the overall incidence and prevalence of the condition are steadily increasing. Medical therapies have proven efficacious, but only a small number of pharmacological options are in development. When patients cease to respond adequately to optimal medical therapy, cardiac resynchronization therapy has been shown to improve symptoms, reduce hospitalizations, promote reverse remodelling, and decrease mortality. However, challenges remain in identifying the ideal recipients for this therapy. The field of mechanical circulatory support has seen immense growth since the early 2000s, and left ventricular assist devices (LVADs) have transitioned over the past decade from large, pulsatile devices to smaller, more-compact, continuous-flow devices. Infections and haematological issues are still important areas that need to be addressed. Whereas LVADs were once approved only for 'bridge to transplantation', these devices are now used as destination therapy for critically ill patients with HF, allowing these individuals to return to the community. A host of novel strategies, including cardiac contractility modulation, implantable haemodynamic-monitoring devices, and phrenic and vagus nerve stimulation, are under investigation and might have an impact on the future care of patients with chronic HF.
Conflict of interest statement
Figures
References
-
- Lloyd-Jones DM, et al. Lifetime risk for developing congestive heart failure: The Framingham Heart Study. Circulation. 2002;106:3068–3072. - PubMed
-
- The SOLVD Investigators. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med. 1992;327:685–691. - PubMed
-
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000;342:145–153. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
