

Clinical outcome and changes in gait pattern after pilon fractures
- PMID: 23229797
- PMCID: PMC3532654
- DOI: 10.1007/s00264-012-1716-1
Clinical outcome and changes in gait pattern after pilon fractures
Abstract
Purpose: Axial burst fractures of the distal tibia are challenging to treat and often lead to restricted function of the lower limb. The purpose of this study was to investigate the clinical outcome and changes in gait pattern in such patients.
Methods: Thirty-five patients in a level 1 trauma centre were followed up clinically and by gait analysis. The American Orthopaedic Foot and Ankle Society (AOFAS), visual analogue scale (VAS) foot and ankle scale and Phillips scores were applied. Dynamic pedography (emed-M; Novel, Germany) with analyses of load, pressure and force-time integral were undertaken to investigate possible changes in gait pattern.
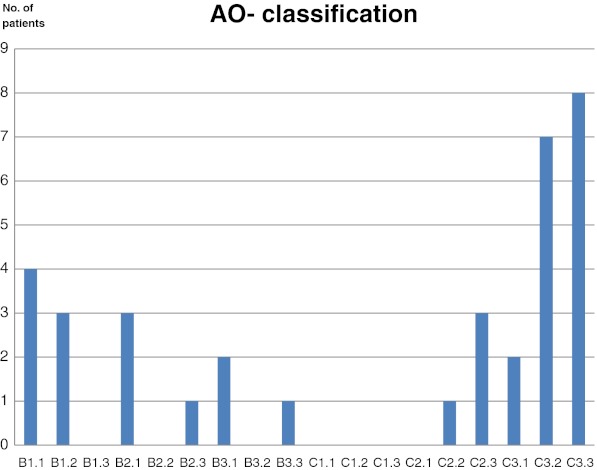
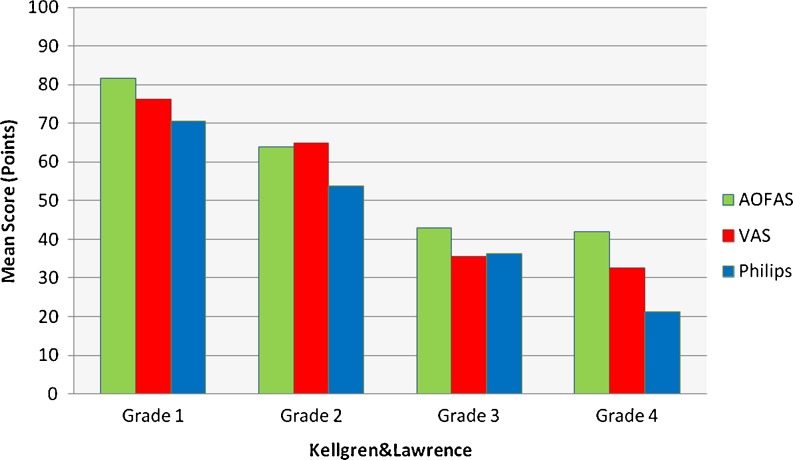
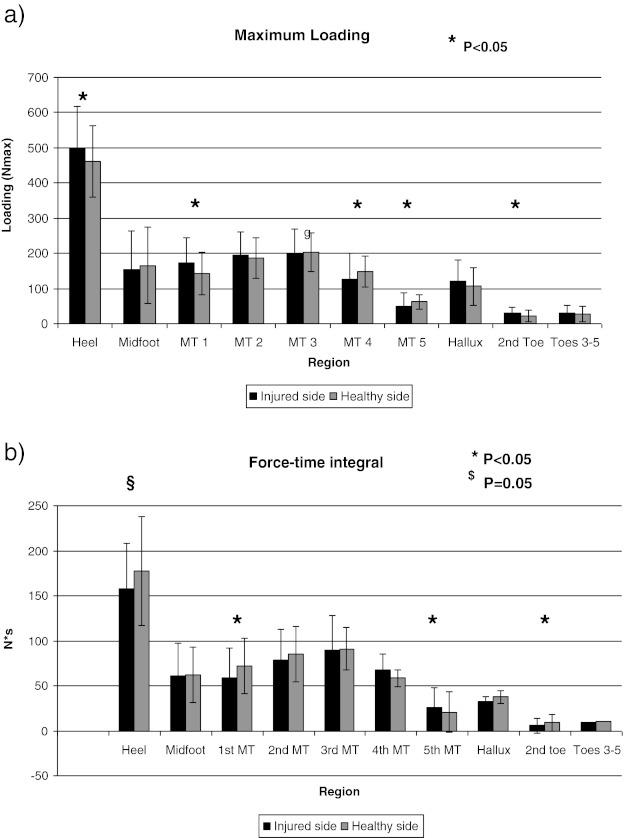
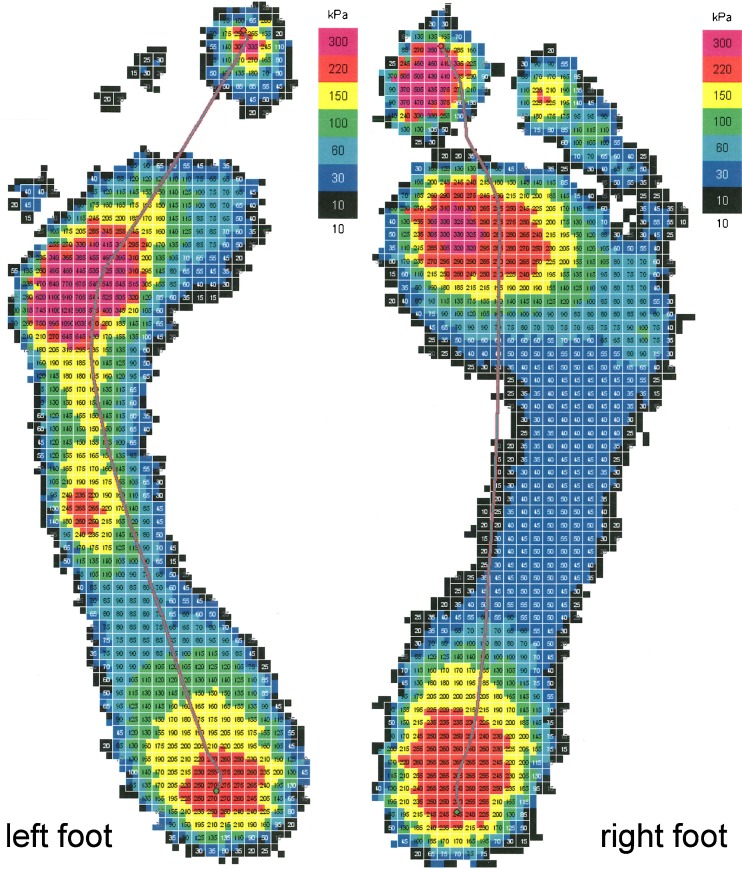
Results: Mean follow-up was 50 (19-100) months. Mean AOFAS, VAS foot and ankle and Phillips scores were 65, 63 and 55 points, respectively. There were clear correlations between fracture severity in the Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification and functional outcome in AOFAS (-0.63; p < 0.01), VAS foot and ankle scale (-0.56; p < 0.01) and Phillips (-0.64; p < 0.01) scores. There was a high correlation of 0.74 (p < 0.01) between the severity of the injury in the AO-classification and onset of post-traumatic arthrosis. Dynamic pedography revealed lesser load bearing for the total foot, medial foot, heel, first metatarsal and medial forefoot for the affected limb, and increased load bearing was seen in the lateral midfoot region.
Conclusions: Fractures of the tibial pilon lead to restricted function of the lower limb. Clinical outcome correlates with fracture severity in the AO classification, the onset of post-traumatic arthrosis and changes in gait patterns.
Figures


Similar articles
-
Distal tibial pilon fractures (AO/OTA type B, and C) treated with the external skeletal and minimal internal fixation method.Vojnosanit Pregl. 2013 Sep;70(9):836-41. doi: 10.2298/vsp1309836m. Vojnosanit Pregl. 2013. PMID: 24266311
-
Staged posterior tibial plating for the treatment of Orthopaedic Trauma Association 43C2 and 43C3 tibial pilon fractures.J Orthop Trauma. 2012 Jun;26(6):341-7. doi: 10.1097/BOT.0b013e318225881a. J Orthop Trauma. 2012. PMID: 22207206
-
Osteochondral autograft transplantation in the treatment of AO/OTA type C3 tibial plafond fractures with irreducibly comminuted area and/or cartilage delamination in the distal tibial facet.Injury. 2022 Apr;53(4):1523-1531. doi: 10.1016/j.injury.2022.01.040. Epub 2022 Jan 26. Injury. 2022. PMID: 35140029
-
Surgical approach strategies for open reduction internal fixation of closed complex tibial Pilon fractures based on axial CT scans.J Orthop Surg Res. 2020 Jul 27;15(1):283. doi: 10.1186/s13018-020-01770-y. J Orthop Surg Res. 2020. PMID: 32718324 Free PMC article.
-
Multi-segment foot kinematics after total ankle replacement and ankle arthrodesis during relatively long-distance gait.Gait Posture. 2012 Jul;36(3):561-6. doi: 10.1016/j.gaitpost.2012.05.010. Epub 2012 Jul 3. Gait Posture. 2012. PMID: 22763319
Cited by
-
Comparison between Exercise Program-Foot Orthoses Treatment and Exercise Program Alone after Pilon Fracture Surgery: Study Protocol for a Randomized Controlled Trial.Life (Basel). 2023 Nov 10;13(11):2187. doi: 10.3390/life13112187. Life (Basel). 2023. PMID: 38004327 Free PMC article.
-
Gait Alterations in Adults after Ankle Fracture: A Systematic Review.Diagnostics (Basel). 2022 Jan 14;12(1):199. doi: 10.3390/diagnostics12010199. Diagnostics (Basel). 2022. PMID: 35054366 Free PMC article. Review.
-
Validation and reliability testing of a new, fully integrated gait analysis insole.J Foot Ankle Res. 2015 Sep 22;8:54. doi: 10.1186/s13047-015-0111-8. eCollection 2015. J Foot Ankle Res. 2015. PMID: 26396594 Free PMC article.
-
Clinical Assessments of Fracture Healing and Basic Science Correlates: Is There Room for Convergence?Curr Osteoporos Rep. 2023 Apr;21(2):216-227. doi: 10.1007/s11914-022-00770-7. Epub 2022 Dec 19. Curr Osteoporos Rep. 2023. PMID: 36534307 Review.
-
Kinematic Parameters Following Pilon Fracture Treatment with the Ilizarov Method.J Clin Med. 2022 May 13;11(10):2763. doi: 10.3390/jcm11102763. J Clin Med. 2022. PMID: 35628891 Free PMC article.
References
-
- Bacon S, Smith WR, Morgan SJ, Hasenboehler E, Philips G, Williams A, Ziran BH, Stahel PF. A retrospective analysis of comminuted intra-articular fractures of the tibial plafond: Open reduction and internal fixation versus external Ilizarov fixation. Injury. 2008;39(2):196–202. doi: 10.1016/j.injury.2007.09.003. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
