

Integrating technology into standard weight loss treatment: a randomized controlled trial
- PMID: 23229890
- PMCID: PMC3684245
- DOI: 10.1001/jamainternmed.2013.1221
Integrating technology into standard weight loss treatment: a randomized controlled trial
Abstract
Background: A challenge in intensive obesity treatment is making care scalable. Little is known about whether the outcome of physician-directed weight loss treatment can be improved by adding mobile technology.
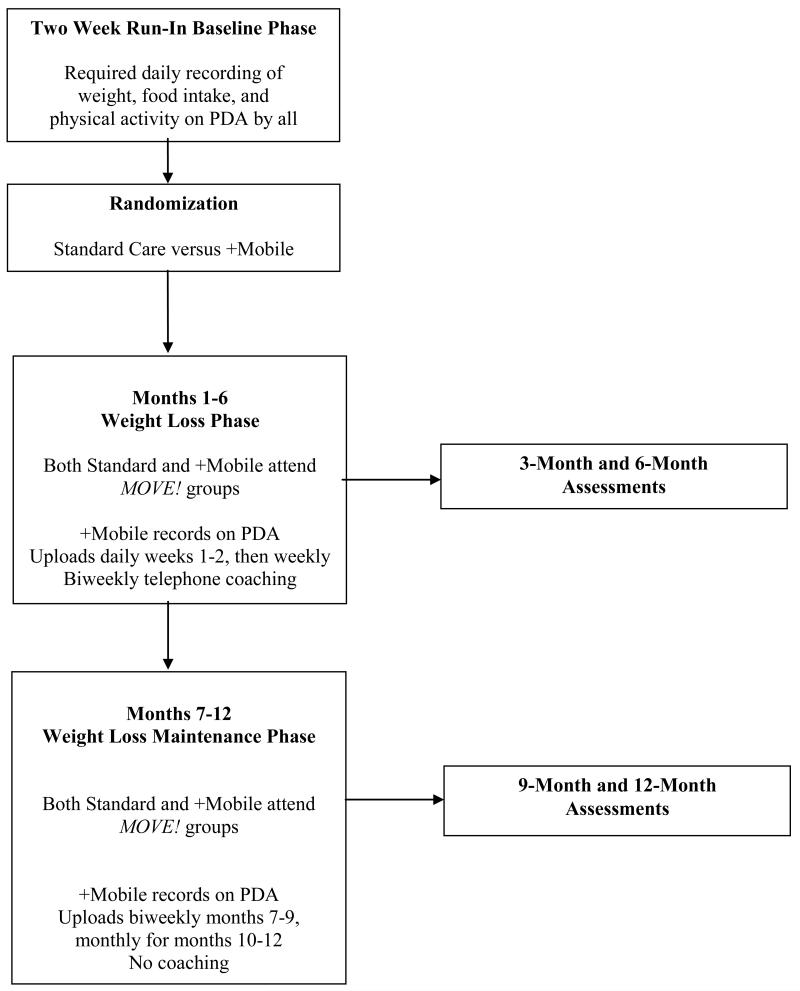
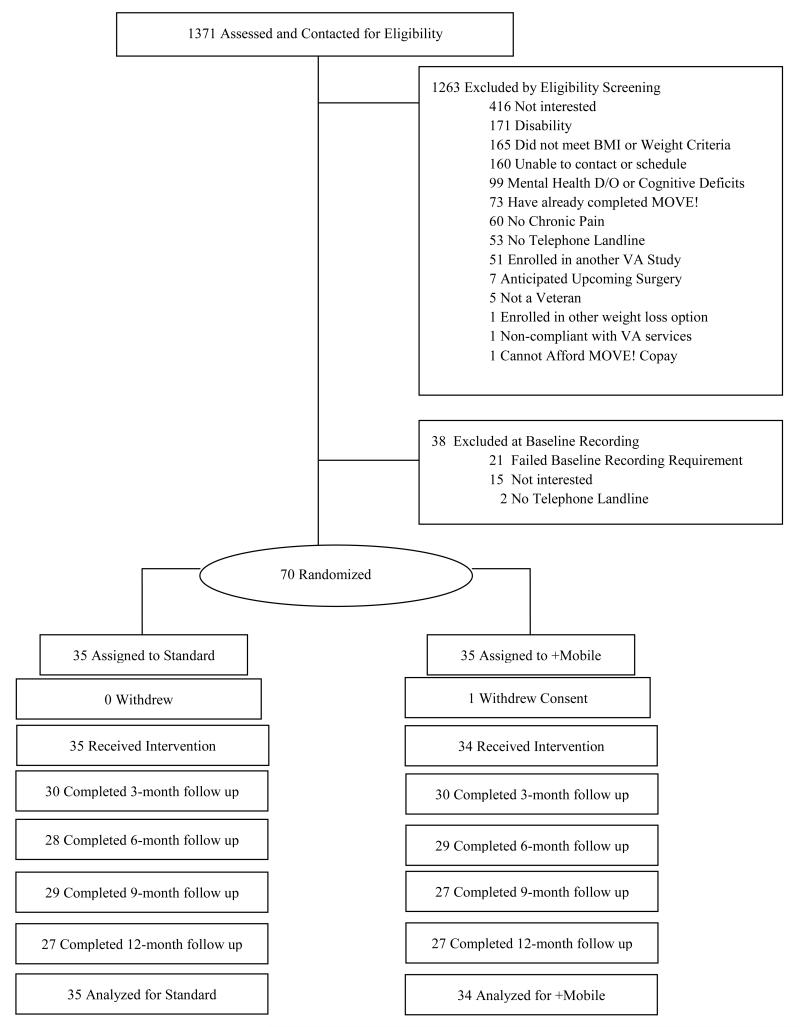
Methods: We conducted a 2-arm, 12-month study (October 1, 2007, through September 31, 2010). Seventy adults (body mass index >25 and ≤40 [calculated as weight in kilograms divided by height in meters squared]) were randomly assigned either to standard-of-care group treatment alone (standard group) or to the standard and connective mobile technology system (+mobile group). Participants attended biweekly weight loss groups held by the Veterans Affairs outpatient clinic. The +mobile group was provided personal digital assistants to self-monitor diet and physical activity; they also received biweekly coaching calls for 6 months. Weight was measured at baseline and at 3-, 6-, 9-, and 12-month follow-up.
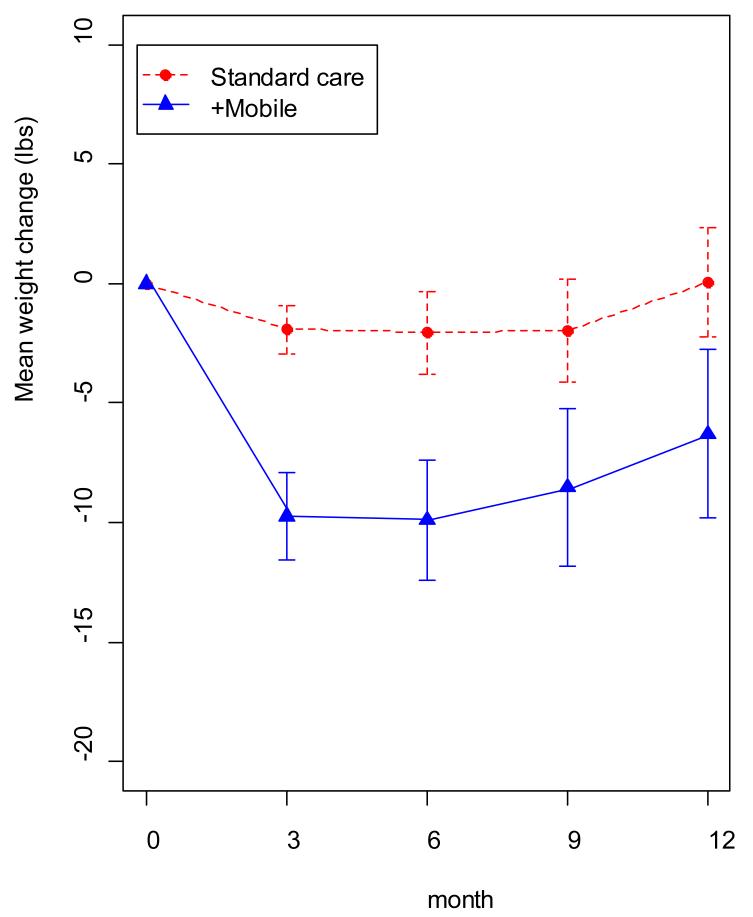
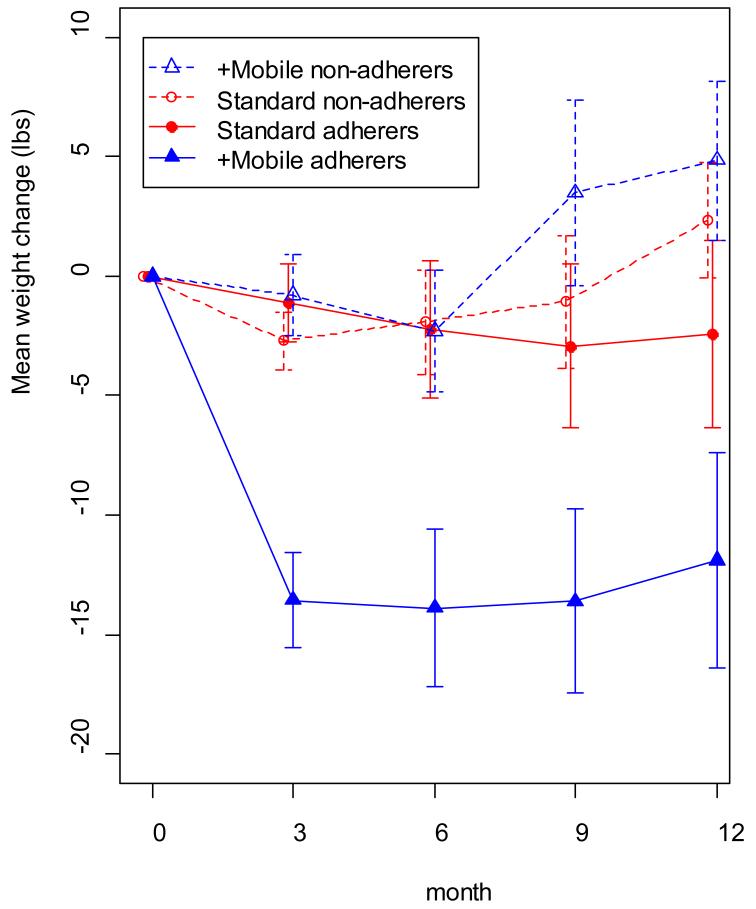
Results: Sixty-nine adults received intervention (mean age, 57.7 years; 85.5% were men). A longitudinal intent-to-treat analysis indicated that the +mobile group lost a mean of 3.9 kg more (representing 3.1% more weight loss relative to the control group; 95% CI, 2.2-5.5 kg) than the standard group at each postbaseline time point. Compared with the standard group, the +mobile group had significantly greater odds of having lost 5% or more of their baseline weight at each postbaseline time point (odds ratio, 6.5; 95% CI, 2.5-18.6).
Conclusions: The addition of a personal digital assistant and telephone coaching can enhance short-term weight loss in combination with an existing system of care. Mobile connective technology holds promise as a scalable mechanism for augmenting the effect of physician-directed weight loss treatment.
Trial registration: clinicaltrials.gov Identifier: NCT00371462.
Figures
Comment in
-
The future of obesity treatment: comment on "Integrating technology into standard weight loss treatment: a randomized controlled trial".JAMA Intern Med. 2013 Jan 28;173(2):111-2. doi: 10.1001/jamainternmed.2013.1232. JAMA Intern Med. 2013. PMID: 23229914 No abstract available.
-
Obesity: finding weight loss strategies that work in primary care.Nat Rev Endocrinol. 2013 Mar;9(3):126. doi: 10.1038/nrendo.2012.244. Epub 2013 Jan 8. Nat Rev Endocrinol. 2013. PMID: 23296170 No abstract available.
References
-
- Franz MJ, VanWormer JJ, Crain AL, et al. Weight loss outcomes: a systematic review and meta-analysis of weight loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc. 2007 Oct;107(10):1755–1767. - PubMed
-
- Wadden TA, Crerand CE, Brock J. Behavioral treatment of obesity. Psychiatr Clin North Am. 2005 Mar;28(1):151–+. - PubMed
-
- Leblanc ES, O’Connor E, Whitlock EP, Patnode CD, Kapka T. Effectiveness of primary care-relevant treatments for obesity in adults: a systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2011 Oct 4;155(7):434–447. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
