

Age- and sex-specific mortality associated with the 1918-1919 influenza pandemic in Kentucky
- PMID: 23230061
- PMCID: PMC3563305
- DOI: 10.1093/infdis/jis745
Age- and sex-specific mortality associated with the 1918-1919 influenza pandemic in Kentucky
Abstract
Background: The reasons for the unusual age-specific mortality patterns of the 1918-1919 influenza pandemic remain unknown. Here we characterize pandemic-related mortality by single year of age in a unique statewide Kentucky data set and explore breakpoints in the age curves.
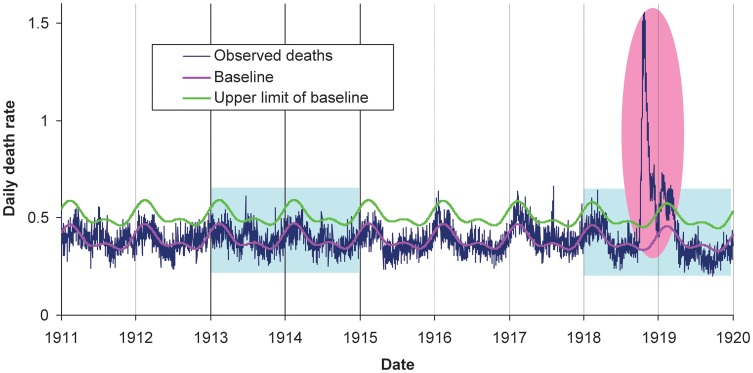
Methods: Individual death certificates from Kentucky during 1911-1919 were abstracted by medically trained personnel. Pandemic-associated excess mortality rates were calculated by subtracting observed rates during pandemic months from rates in previous years, separately for each single year of age and by sex.
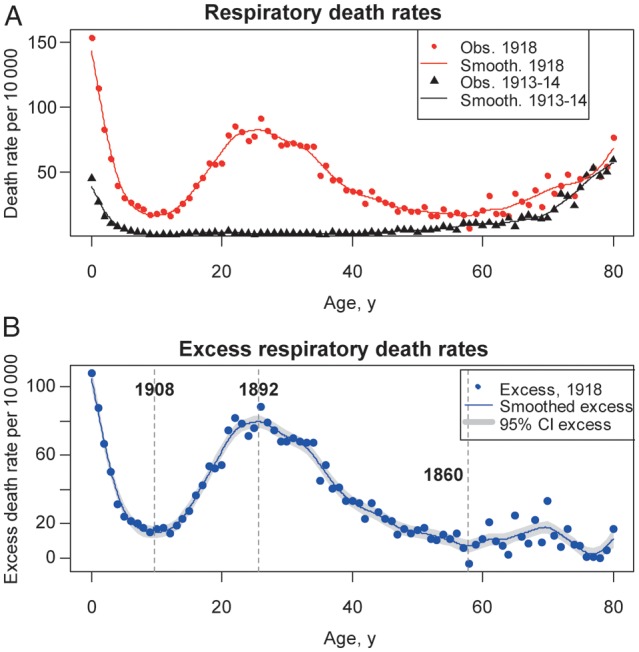
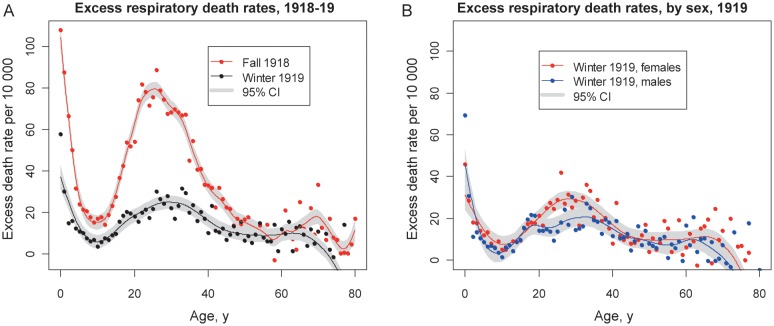
Results: The age profile of excess mortality risk in fall 1918 was characterized by a maximum among infants, a minimum at ages 9-10 years, a maximum at ages 24-26 years, and a second minimum at ages 56-59 years. The excess mortality risk in young adults had been greatly attenuated by winter 1919. The age breakpoints of mortality risk did not differ between males and females.
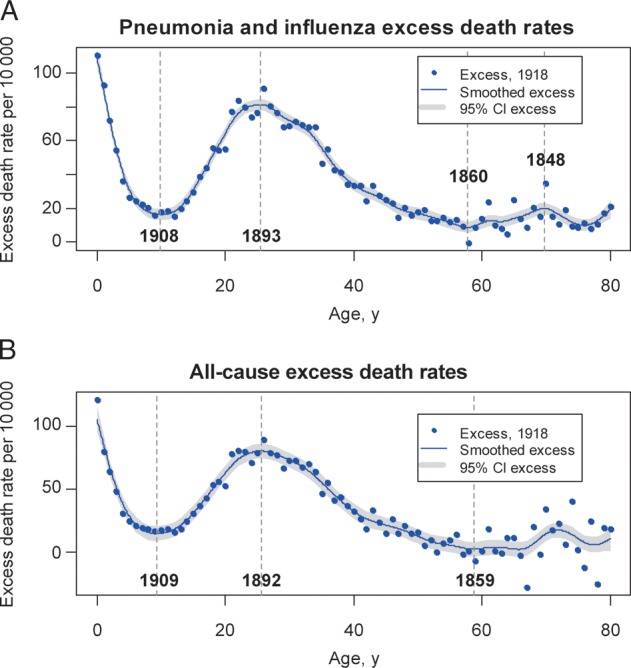
Conclusions: The observed mortality breakpoints in male and female cohorts born during 1859-1862, 1892-1894, and 1908-1909 did not coincide with known dates of historical pandemics. The atypical age mortality patterns of the 1918-1919 pandemic cannot be explained by military crowding, war-related factors, or prior immunity alone and likely result from a combination of unknown factors.
Figures


Comment in
-
Age-specific mortality during the 1918-19 influenza pandemic and possible relationship to the 1889-92 influenza pandemic.J Infect Dis. 2014 Sep 15;210(6):993-5. doi: 10.1093/infdis/jiu191. Epub 2014 Mar 27. J Infect Dis. 2014. PMID: 24676203 No abstract available.
-
Reply to Wilson et al.J Infect Dis. 2014 Sep 15;210(6):995-7. doi: 10.1093/infdis/jiu192. Epub 2014 Mar 27. J Infect Dis. 2014. PMID: 24676205 Free PMC article. No abstract available.
References
-
- Johnson NP, Mueller J. Updating the accounts: global mortality of the 1918–20 “Spanish” influenza epidemic. Bull Hist Med. 2002;76:105–15. - PubMed
-
- Murray CJ, Lopez AD, Chin B, Feehan D, Hill KH. Estimation of potential global pandemic influenza mortality on the basis of vital registry data from the 1918–20 pandemic: a quantitative analysis. Lancet. 2006;368:2211–8. - PubMed
-
- Miller MA, Viboud C, Balinska M, Simonsen L. The signature features of influenza pandemics—implications for policy. N Engl J Med. 2009;360:2595–8. - PubMed
-
- Jordan EO. Epidemic influenza. Chicago: American Medical Association; 1927.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
