

Improving situation awareness to reduce unrecognized clinical deterioration and serious safety events
- PMID: 23230078
- PMCID: PMC4528338
- DOI: 10.1542/peds.2012-1364
Improving situation awareness to reduce unrecognized clinical deterioration and serious safety events
Abstract
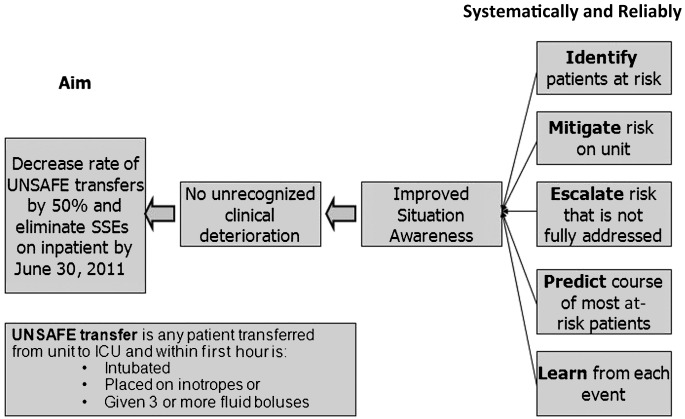
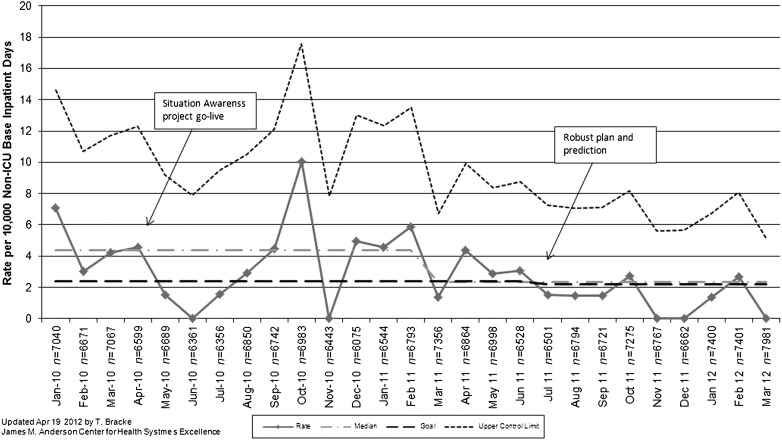
Background and objective: Failure to recognize and treat clinical deterioration remains a source of serious preventable harm for hospitalized patients. We designed a system to identify, mitigate, and escalate patient risk by using principles of high-reliability organizations. We hypothesized that our novel care system would decrease transfers determined to be unrecognized situation awareness failures events (UNSAFE). These were defined as any transfer from an acute care floor to an ICU where the patient received intubation, inotropes, or ≥ 3 fluid boluses in first hour after arrival or before transfer.
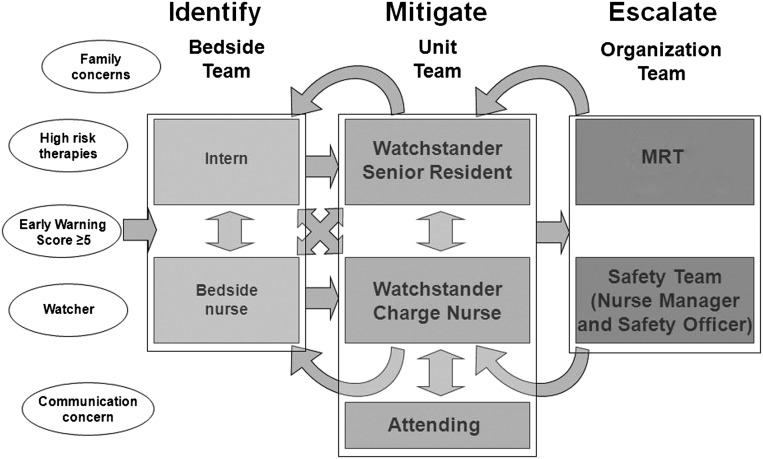
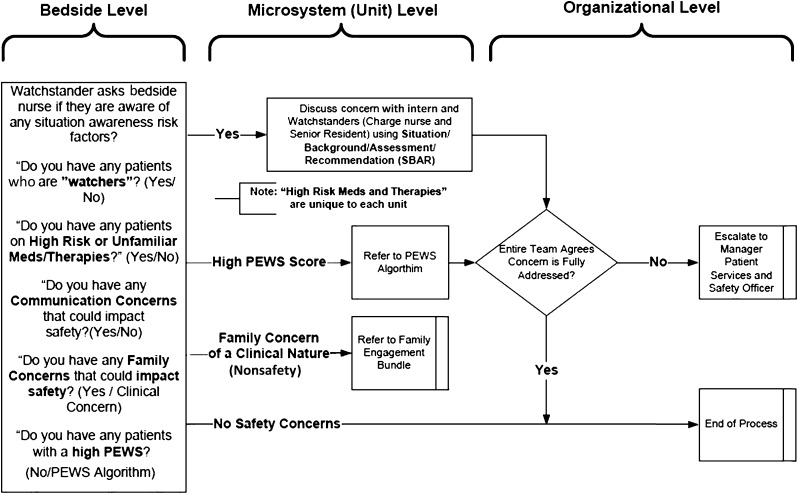
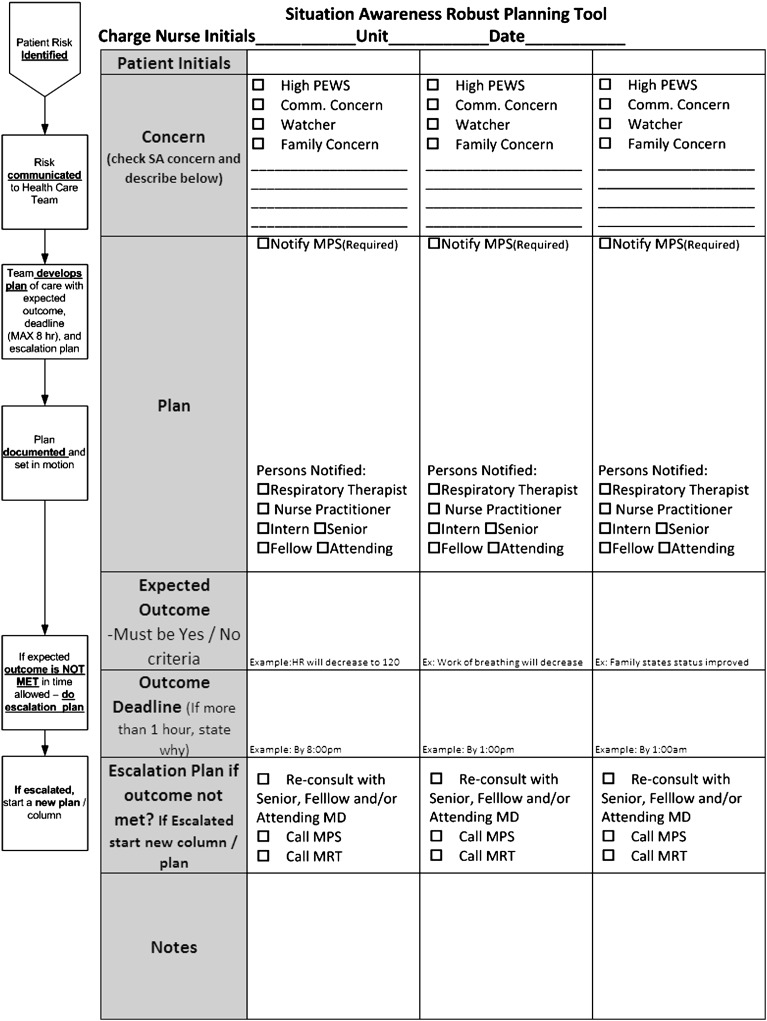
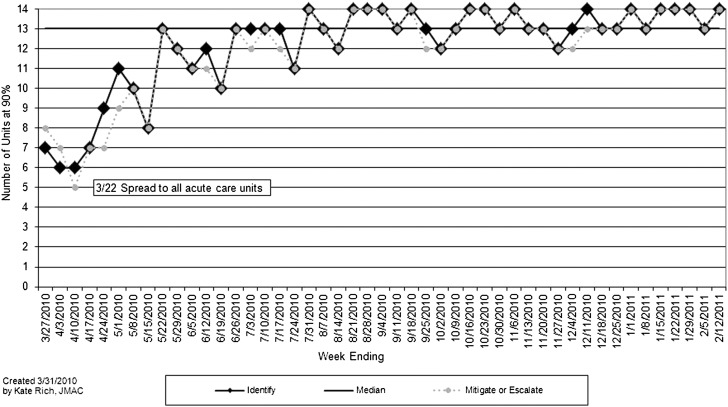
Methods: The setting for our observational time series study was a quaternary care children's hospital. Before initiating tests of change, 2 investigators reviewed recent serious safety events (SSEs) and floor-to-ICU transfers. Collectively, 5 risk factors were associated with each event: family concerns, high-risk therapies, presence of an elevated early warning score, watcher/clinician gut feeling, and communication concerns. Using the model for improvement, an intervention was developed and tested to reliably and proactively identify patient risk and mitigate that risk through unit-based huddles. A 3-times daily inpatient huddle was added to ensure risks were escalated and addressed. Later, a "robust" and explicit plan for at-risk patients was developed and spread.
Results: The rate of UNSAFE transfers per 10,000 non-ICU inpatient days was significantly reduced from 4.4 to 2.4 over the study period. The days between inpatient SSEs also increased significantly.
Conclusions: A reliable system to identify, mitigate, and escalate risk was associated with a near 50% reduction in UNSAFE transfers and SSEs.
Figures
Comment in
-
Situation awareness: a new model for predicting and preventing patient deterioration.Hosp Pediatr. 2014 May;4(3):143-6. doi: 10.1542/hpeds.2013-0119. Hosp Pediatr. 2014. PMID: 24785557 No abstract available.
References
-
- Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C. Rapid response teams: a systematic review and meta-analysis. Arch Intern Med. 2010;170(1):18–26 - PubMed
-
- Brilli RJ, Gibson R, Luria JW, et al. Implementation of a medical emergency team in a large pediatric teaching hospital prevents respiratory and cardiopulmonary arrests outside the intensive care unit. Pediatr Crit Care Med. 2007;8(3):236–246, quiz 247 - PubMed
-
- Sharek PJ, Parast LM, Leong K, et al. Effect of a rapid response team on hospital-wide mortality and code rates outside the ICU in a children’s hospital. JAMA. 2007;298(19):2267–2274 - PubMed
-
- Van Voorhis KT, Willis TS. Implementing a pediatric rapid response system to improve quality and patient safety. Pediatr Clin North Am. 2009;56(4):919–933 - PubMed
-
- Hillman KM, Bristow PJ, Chey T, et al. Duration of life-threatening antecedents prior to intensive care admission. Intensive Care Med. 2002;28(11):1629–1634 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
