

The clinical usefulness of extravascular lung water and pulmonary vascular permeability index to diagnose and characterize pulmonary edema: a prospective multicenter study on the quantitative differential diagnostic definition for acute lung injury/acute respiratory distress syndrome
- PMID: 23232188
- PMCID: PMC3672621
- DOI: 10.1186/cc11898
The clinical usefulness of extravascular lung water and pulmonary vascular permeability index to diagnose and characterize pulmonary edema: a prospective multicenter study on the quantitative differential diagnostic definition for acute lung injury/acute respiratory distress syndrome
Abstract
Introduction: Acute lung injury (ALI)/acute respiratory distress syndrome (ARDS) is characterized by features other than increased pulmonary vascular permeability. Pulmonary vascular permeability combined with increased extravascular lung water content has been considered a quantitative diagnostic criterion of ALI/ARDS. This prospective, multi-institutional, observational study aimed to clarify the clinical pathophysiological features of ALI/ARDS and establish its quantitative diagnostic criteria.
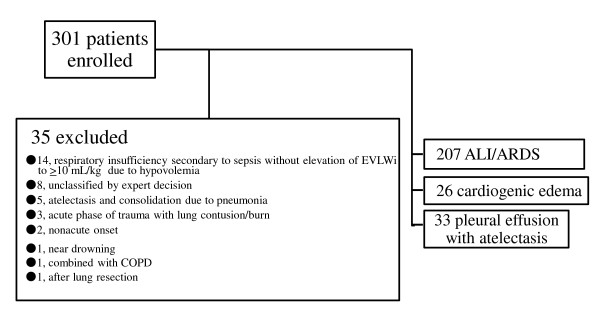
Methods: The extravascular lung water index (EVLWI) and the pulmonary vascular permeability index (PVPI) were measured using the transpulmonary thermodilution method in 266 patients with PaO2/FiO2 ratio ≤ 300 mmHg and bilateral infiltration on chest radiography, in 23 ICUs of academic tertiary referral hospitals. Pulmonary edema was defined as EVLWI ≥ 10 ml/kg. Three experts retrospectively determined the pathophysiological features of respiratory insufficiency by considering the patients' history, clinical presentation, chest computed tomography and radiography, echocardiography, EVLWI and brain natriuretic peptide level, and the time course of all preceding findings under systemic and respiratory therapy.
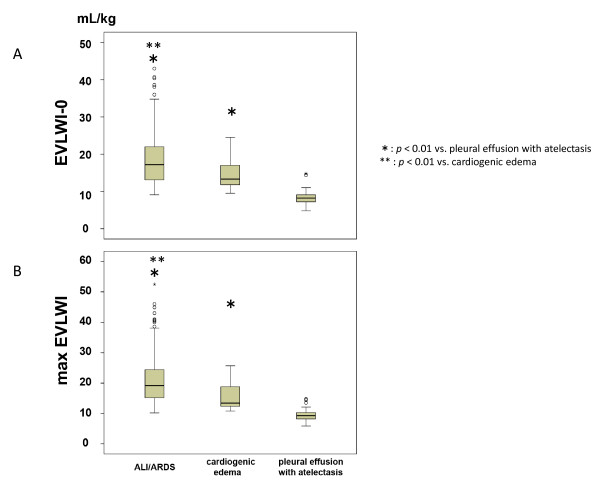
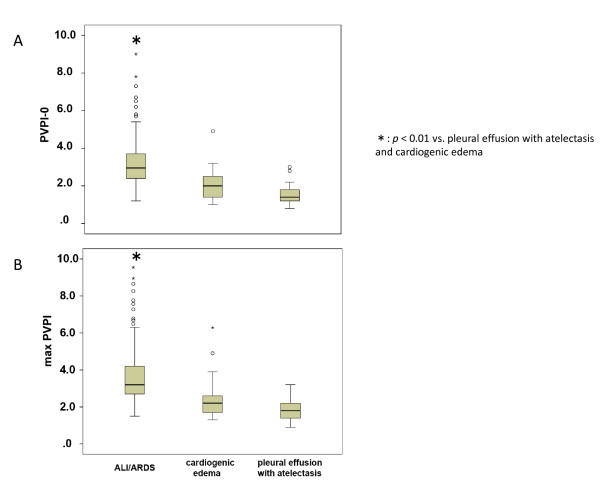
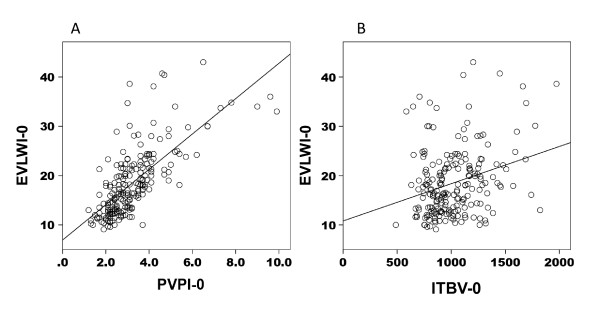
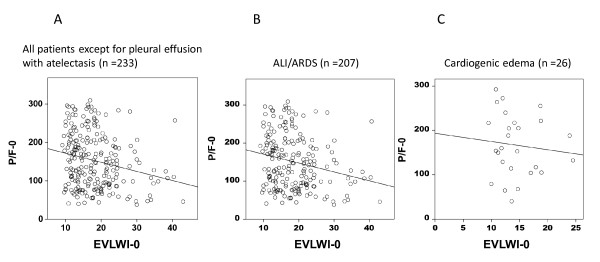
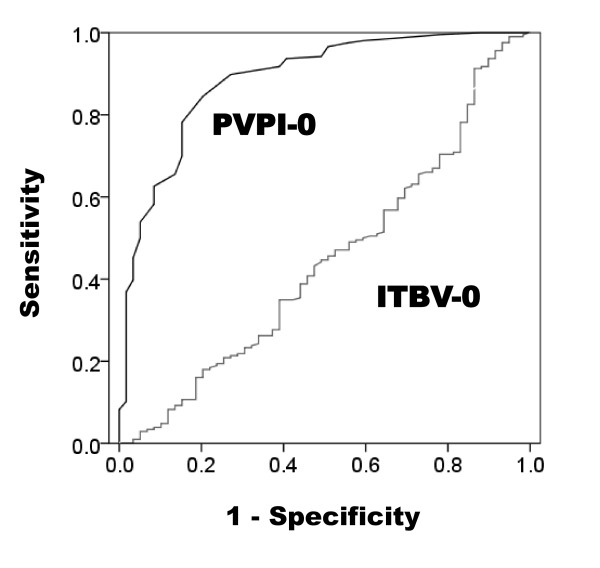
Results: Patients were divided into the following three categories on the basis of the pathophysiological diagnostic differentiation of respiratory insufficiency: ALI/ARDS, cardiogenic edema, and pleural effusion with atelectasis, which were noted in 207 patients, 26 patients, and 33 patients, respectively. EVLWI was greater in ALI/ARDS and cardiogenic edema patients than in patients with pleural effusion with atelectasis (18.5 ± 6.8, 14.4 ± 4.0, and 8.3 ± 2.1, respectively; P < 0.01). PVPI was higher in ALI/ARDS patients than in cardiogenic edema or pleural effusion with atelectasis patients (3.2 ± 1.4, 2.0 ± 0.8, and 1.6 ± 0.5; P < 0.01). In ALI/ARDS patients, EVLWI increased with increasing pulmonary vascular permeability (r = 0.729, P < 0.01) and was weakly correlated with intrathoracic blood volume (r = 0.236, P < 0.01). EVLWI was weakly correlated with the PaO2/FiO2 ratio in the ALI/ARDS and cardiogenic edema patients. A PVPI value of 2.6 to 2.85 provided a definitive diagnosis of ALI/ARDS (specificity, 0.90 to 0.95), and a value < 1.7 ruled out an ALI/ARDS diagnosis (specificity, 0.95).
Conclusion: PVPI may be a useful quantitative diagnostic tool for ARDS in patients with hypoxemic respiratory failure and radiographic infiltrates.
Trial registration: UMIN-CTR ID UMIN000003627.
Figures

Comment in
-
Extravascular lung water and the pulmonary vascular permeability index may improve the definition of ARDS.Crit Care. 2013 Jan 24;17(1):108. doi: 10.1186/cc11918. Crit Care. 2013. PMID: 23347799 Free PMC article.
-
A bedside definition of acute respiratory distress syndrome based on a conceptual model.Crit Care. 2013 Mar 14;17(2):418. doi: 10.1186/cc12539. Crit Care. 2013. PMID: 23509995 Free PMC article. No abstract available.
-
Extravascular lung water and pulmonary vascular permeability index may inadvertently delay the identification of acute respiratory distress syndrome.Crit Care. 2013 Mar 20;17(2):420. doi: 10.1186/cc12542. Crit Care. 2013. PMID: 23522053 Free PMC article. No abstract available.
-
Author's response.Crit Care. 2013;17(2):418. Crit Care. 2013. PMID: 25232575 No abstract available.
-
Authors' response.Crit Care. 2013;17(2):420. Crit Care. 2013. PMID: 25232576 No abstract available.
References
-
- Meade MO, Cook RJ, Guyatt GH, Groll R, Kachura JR, Bedard M, Cook DJ, Slutsky AS, Stewart TE. Interobserver variation in interpreting chest radiographs for the diagnosis of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2000;16:85–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
