

Use of advanced imaging technology and endoscopy for chronic rhinosinusitis varies by physician specialty
- PMID: 23232199
- PMCID: PMC3972731
- DOI: 10.2500/ajra.2012.26.3817
Use of advanced imaging technology and endoscopy for chronic rhinosinusitis varies by physician specialty
Abstract
Background: Patients with chronic rhinosinusitis are cared for by multiple specialties. Endoscopy and imaging are important diagnostic tools. However, because physicians vary in their access to imaging and endoscopy, testing may vary across specialties. The purpose of this study is to characterize differences in use of imaging and endoscopy between physician specialties.
Methods: Using data from the National Ambulatory Medical Care Survey, we identified adult visits with primary, secondary, and tertiary diagnoses of chronic rhinosinusitis from 2005 through 2008. We measured rates of advanced radiographic imaging (CT, MRI, and PET) and office procedures. Logistic regression models were used to assess the bivariate and independent effects of patient, physician, and practice-level factors on use of advanced imaging and office procedures.
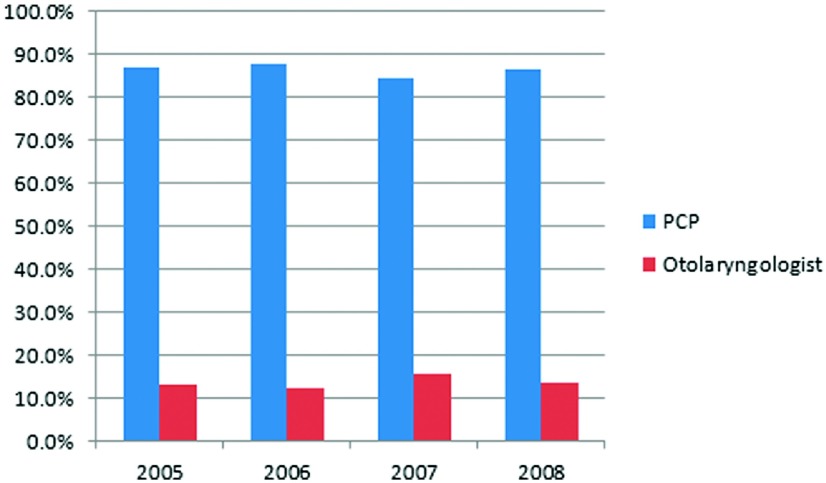
Results: There were nearly 51 million visits for diagnoses coded as chronic rhinosinusitis, representing an average of 12.7 million visits annually. Primary care providers saw the majority of these patients. Otolaryngologists used advanced radiographic imaging at a rate higher than primary care physicians per outpatient visit (16.0% versus 1.93%; p < 0.001). Office procedures, performed almost exclusively (99.2%) by otolaryngologists, were performed at 24.5% of otolaryngology visits. Private insurance was significantly associated with a lower use of advanced radiographic imaging (odds ratio, 0.54; 95% CI, 0.31-0.94) among otolaryngology visits, but no patient or provider-level variables were associated with office procedure use.
Conclusion: Radiographic imaging and office procedures are used at a higher rate per outpatient visit by otolaryngologists than by primary care providers. Additional studies are needed to identify and characterize factors that contribute to these different rates of use.
Conflict of interest statement
The authors have no conflicts of interest to declare pertaining to this article
Figures
References
-
- Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg 137(suppl):S1–S31, 2007. - PubMed
-
- Anand VK. Epidemiology and economic impact of rhinosinusitis. Ann Otol Rhinol Laryngol Suppl 193:3–5, 2004. - PubMed
-
- Pleis JR, Lethbridge-Cejku M. Summary health statistics for U.S. adults: National Health Interview Survey, 2006. Vital Health Stat 10:1–153, 2007. - PubMed
-
- Sinus and Allergy Health Partnership. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg 130(suppl):1–45, 2004. - PubMed
-
- Ray NF, Baraniuk JN, Thamer M, et al. Healthcare expenditures for sinusitis in 1996: Contributions of asthma, rhinitis, and other airway disorders. J Allergy Clin Immunol 103:408–414, 1999. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
