

Hyperbaric oxygen therapy for the adjunctive treatment of traumatic brain injury
- PMID: 23235612
- PMCID: PMC11561354
- DOI: 10.1002/14651858.CD004609.pub3
Hyperbaric oxygen therapy for the adjunctive treatment of traumatic brain injury
Abstract
Background: Traumatic brain injury is a common health problem with significant effect on quality of life. Each year in the USA approximately 0.56% of the population suffer a head injury, with a case fatality rate of about 40% for severe injuries. These account for a high proportion of deaths in young adults. In the USA, 2% of the population live with long-term disabilities following head injuries. The major causes are motor vehicle crashes, falls, and violence (including attempted suicide). Hyperbaric oxygen therapy (HBOT) is the therapeutic administration of 100% oxygen at environmental pressures greater than 1 atmosphere absolute (ATA). This involves placing the patient in an airtight vessel, increasing the pressure within that vessel, and administering 100% oxygen for respiration. In this way, it is possible to deliver a greatly increased partial pressure of oxygen to the tissues. HBOT can improve oxygen supply to the injured brain, reduce the swelling associated with low oxygen levels and reduce the volume of brain that will ultimately perish. It is, therefore, possible that adding HBOT to the standard intensive care regimen may reduce patient death and disability. However, a concern for patients and families is that using HBOT may result in preventing a patient from dying only to leave them in a vegetative state, entirely dependent on medical care. There are also some potential adverse effects of the therapy, including damage to the ears, sinuses and lungs from the effects of the pressure and oxygen poisoning, so the benefits and risks of the therapy need to be carefully evaluated.
Objectives: To assess the effects of adjunctive HBOT for traumatic brain injury.
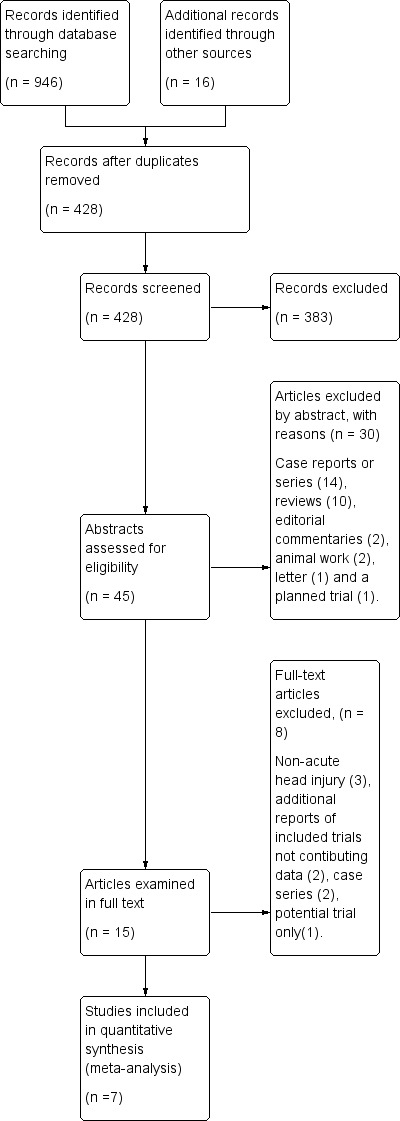
Search methods: We searched CENTRAL, MEDLINE, EMBASE, CINAHL and DORCTHIM electronic databases. We also searched the reference lists of eligible articles, handsearched relevant journals and contacted researchers. All searches were updated to March 2012.
Selection criteria: Randomised studies comparing the effect of therapeutic regimens which included HBOT with those that did not, for people with traumatic brain injury.
Data collection and analysis: Three authors independently evaluated trial quality and extracted data.
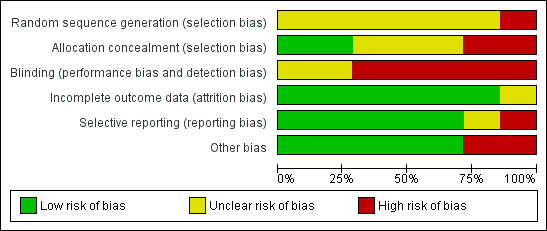
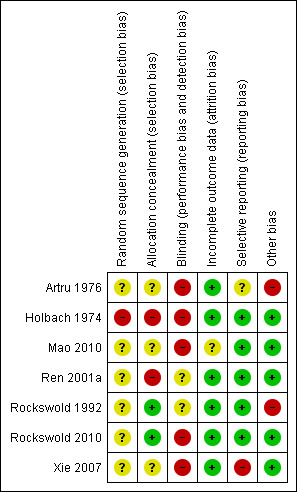
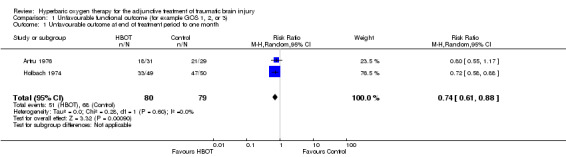
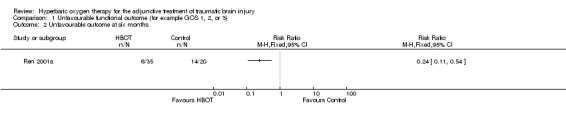
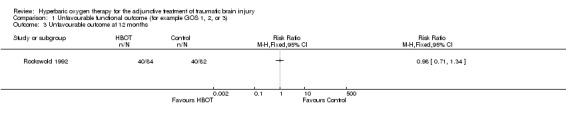
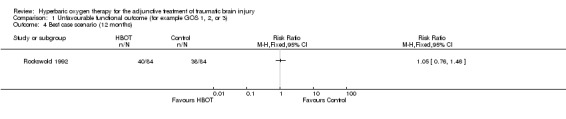
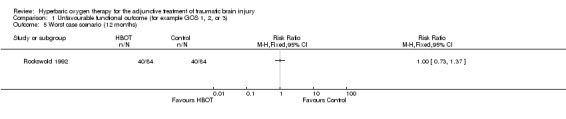
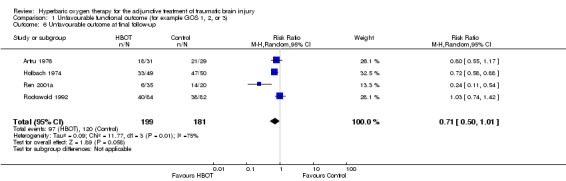
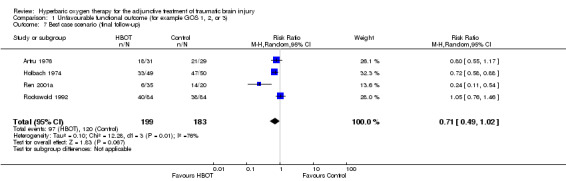
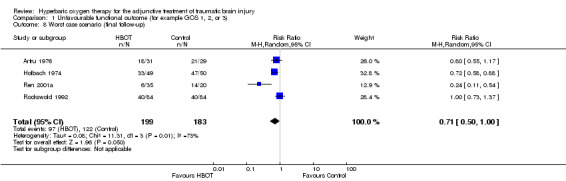
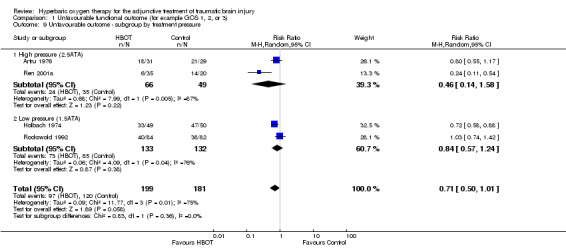
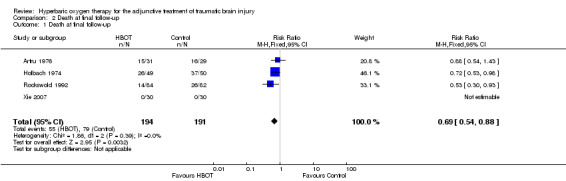
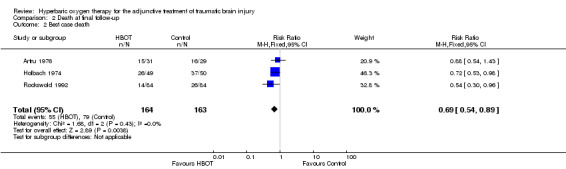
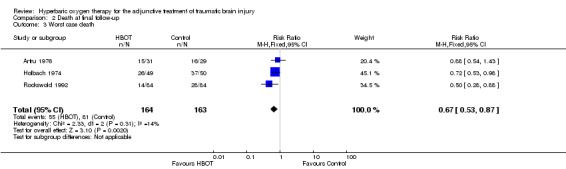
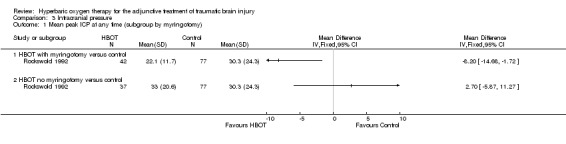
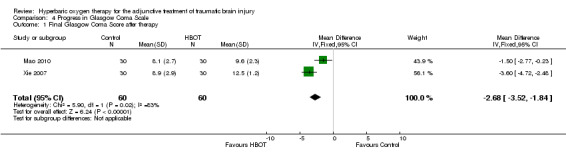
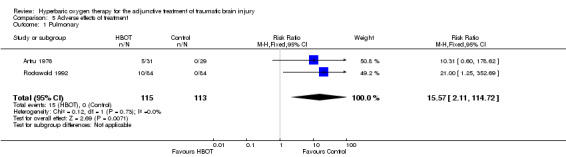
Main results: Seven studies are included in this review, involving 571 people (285 receiving HBOT and 286 in the control group). The results of two studies indicate use of HBOT results in a statistically significant decrease in the proportion of people with an unfavourable outcome one month after treatment using the Glasgow Outcome Scale (GOS) (relative risk (RR) for unfavourable outcome with HBOT 0.74, 95% CI 0.61 to 0.88, P = 0.001). This five-point scale rates the outcome from one (dead) to five (good recovery); an 'unfavourable' outcome was considered as a score of one, two or three. Pooled data from final follow-up showed a significant reduction in the risk of dying when HBOT was used (RR 0.69, 95% CI 0.54 to 0.88, P = 0.003) and suggests we would have to treat seven patients to avoid one extra death (number needed to treat (NNT) 7, 95% CI 4 to 22). Two trials suggested favourably lower intracranial pressure in people receiving HBOT and in whom myringotomies had been performed. The results from one study suggested a mean difference (MD) with myringotomy of -8.2 mmHg (95% CI -14.7 to -1.7 mmHg, P = 0.01). The Glasgow Coma Scale (GCS) has a total of 15 points, and two small trials reported a significant improvement in GCS for patients treated with HBOT (MD 2.68 points, 95%CI 1.84 to 3.52, P < 0.0001), although these two trials showed considerable heterogeneity (I(2) = 83%). Two studies reported an incidence of 13% for significant pulmonary impairment in the HBOT group versus 0% in the non-HBOT group (P = 0.007).In general, the studies were small and carried a significant risk of bias. None described adequate randomisation procedures or allocation concealment, and none of the patients or treating staff were blinded to treatment.
Authors' conclusions: In people with traumatic brain injury, while the addition of HBOT may reduce the risk of death and improve the final GCS, there is little evidence that the survivors have a good outcome. The improvement of 2.68 points in GCS is difficult to interpret. This scale runs from three (deeply comatose and unresponsive) to 15 (fully conscious), and the clinical importance of an improvement of approximately three points will vary dramatically with the starting value (for example an improvement from 12 to 15 would represent an important clinical benefit, but an improvement from three to six would leave the patient with severe and highly dependent impairment). The routine application of HBOT to these patients cannot be justified from this review. Given the modest number of patients, methodological shortcomings of included trials and poor reporting, the results should be interpreted cautiously. An appropriately powered trial of high methodological rigour is required to define which patients, if any, can be expected to benefit most from HBOT.
Conflict of interest statement
None known.
Figures
Update of
-
Hyperbaric oxygen therapy for the adjunctive treatment of traumatic brain injury.Cochrane Database Syst Rev. 2004 Oct 18;(4):CD004609. doi: 10.1002/14651858.CD004609.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2012 Dec 12;12:CD004609. doi: 10.1002/14651858.CD004609.pub3. PMID: 15495120 Updated.
References
References to studies included in this review
Artru 1976 {published data only}
-
- Artru F, Chacornac R, Deleuze R. Hyperbaric oxygenation for severe head injuries. Preliminary results of a controlled study. European Neurology 1976;14(4):310‐8. - PubMed
Holbach 1974 {published data only}
-
- Holbach KH, Wassmann H, Kolberg T. Improved reversibility of the traumatic midbrain syndrome using hyperbaric oxygen. Acta Neurochirurgica (Wien) 1974;30(3‐4):247‐56. [PUBMED: 4432786] - PubMed
Mao 2010 {published data only}
-
- Mao J‐H, Sun Z‐S, Xiang Y. Observation of curative effects of hyperbaric oxygen for treatment on severe craniocerebral injury. Journal of Clinical Neurology 2010;23(5):386‐8.
Ren 2001a {published data only}
-
- Ren H, Wang W, Ge Z. Glasgow coma scale, brain electrical activity mapping and Glasgow outcome score after hyperbaric oxygen treatment of severe brain injury. Chinese Journal of Traumatology 2001;4(4):239‐41. [PUBMED: 11835741] - PubMed
Rockswold 1992 {published data only}
-
- Rockswold GL, Ford SE, Anderson DC, Bergman TA, Sherman RE. Results of a prospective randomized trial for treatment of severely brain‐injured patients with hyperbaric oxygen. Journal of Neurosurgery 1992;76(6):929‐34. [PUBMED: 1588426] - PubMed
Rockswold 2010 {published data only}
-
- Rockswold SB, Rockswold GL, Zaun DA, Zhang X, Cerra CE, Bergman TA, Liu J. A prospective, randomized clinical trial to compare the effect of hyperbaric to normobaric hyperoxia on cerebral metabolism, intracranial pressure, and oxygen toxicity in severe traumatic brain injury. Journal of Neurosurgery 2010;112:1080‐94. - PubMed
Xie 2007 {published data only}
-
- Xie Z, Zhuang M, Lin L, Xu H, Chen L, Hu L. Changes of plasma C‐reactive protein in patients with craniocerebral injury before and after hyperbaric oxygenation: a randomly controlled study. Neural Regeneration Research 2007;2(5):314‐7.
References to studies excluded from this review
Belokurov 1988 {published data only}
-
- Belokurov YM, Golland AV, Kochetov Kh A. Hyperbaric oxygenation in hypoxic brain injuries. Khirurgiya 1988;64(8):104‐6. - PubMed
Gossett 2010 {published data only}
-
- Gossett WA, Rockswold GL, Rockswold SB, Adkinson CD, Bergman TA, Quickel RR. The safe treatment, monitoring and management of severe traumatic brain injury patients in a monoplace chamber. Undersea and Hyperbaric Medicine 2010;37(1):35‐48. - PubMed
Helms 2011 {published data only}
-
- Helms A, Evans AW, Chu J, Sahgal A, Ostrowski R, Sosiak T, Wolf G, Gillett J, Whelan H. Hyperbaric oxygen for neurologic indications‐‐action plan for multicenter trials in: stroke, traumatic brain injury, radiation encephalopathy & status migrainosus. Undersea and Hyperbaric Medicine 2011;38(5):309‐19. - PubMed
Lin 2008 {published data only}
-
- Lin JW, Tsai JT, Lee LM, Lin CM, Hung CC, Hung KS, et al. Effect of hyperbaric oxygen on patients with traumatic brain injury. Acta Neurochirurgica 2008;101 Suppl:145‐9. - PubMed
Ren 2001b {published data only}
-
- Ren H, Wang W, Ge Z. Clinical, Glasgow coma scale, brain electric earth map, endothelin and transcranial ultrasonic doppler findings after hyperbaric oxygen treatment for severe brain injury. Chinese Medical Journal (English) 2001;114(4):387‐90. [PUBMED: 11835741] - PubMed
Rockswold 1985 {published data only}
-
- Rockswold GL, Ford SE. Preliminary results of a prospective randomized trial of treatment of severely brain‐injured patients with hyperbaric oxygen. Minnesota Medical Journal 1985;68(7):533‐5. - PubMed
Shi 2003 {published data only}
-
- Shi XY, Tang ZQ, Xiong B, Bao JX, Sun D, Zhang YQ, et al. Cerebral perfusion SPECT imaging for assessment of the effect of hyperbaric oxygen therapy on patients with postbrain injury neural status. Chinese Journal of Traumatology 2003;6(6):346‐9. [PUBMED: 14642054] - PubMed
Shi 2006 {published data only}
-
- Shi XY, Tang ZQ, Sun D, He XJ. Evaluation of hyperbaric oxygen treatment of neuropsychiatric disorders following traumatic brain injury. Chinese Medical Journal 2006;119(23):1978‐82. - PubMed
Additional references
Adamides 2006
-
- Adamides AA, Winter CD, Lewis PM, Cooper DJ, Kossmann T, Rosenfeld JV. Current controversies in the management of patients with severe traumatic brain injury. Australia and New Zealand Journal of Surgery 2006;76(3):163‐74. - PubMed
Adriessen 2011
-
- Andriessen TMJC, Horn J, Franschman G, Naalt J, Haitsma I, Jacobs B, Steyerberg EW, Vos PE. Epidemiology, severity classification, and outcome of moderate and severe traumatic brain injury: A prospective multicenter study. Journal of Neurotrauma 2011;28(10):2011‐34. [DOI: 10.1089/neu.2011.2034] - DOI - PubMed
Alderson 2008
Alexander 1992
-
- Alexander E. Global Spine and Head Injury Prevention Project (SHIP). Surgical Neurology 1992;38(6):478‐9. [MEDLINE: ] - PubMed
Ali Wali 2005
-
- Al‐Waili NS, Butler GJ, Beale J, Abdullah MS, Hamilton RW, Lee BY, Lucus P, Allen MW, Petrillo RL, Carrey Z, Finkelstein M. Hyperbaric oxygen in the treatment of patients with cerebral stroke, brain trauma, and neurologic disease. Advances in Therapeutics 2005;22(6):659‐78. - PubMed
Alternative Therapy Committee 2003
-
- Alternative Therapy Evaluation Committee for the Insurance Corporation of British Columbia. A review of the scientific evidence on the treatment of traumatic brain injuries and strokes with hyperbaric oxygen. Brain Injury 2003;17(3):225‐36. - PubMed
Artru 1976a
-
- Artru F, Philippon B, Gau F, Berger M, Deleuze R. Cerebral blood flow, cerebral metabolism and cerebrospinal fluid biochemistry in brain‐injured patients after exposure to hyperbaric oxygen. European Neurology 1976;14(5):351‐64. - PubMed
Clark 1982
-
- Clark JM. Oxygen toxicity. In: Bennett PB, Elliott DH editor(s). The Physiology and Medicine of Diving. 3rd Edition. London: Bailliere, Tindall and Cox, 1982:200‐38.
Fasano 1964
-
- Fasano VA, Nunno T, Urciolo R, Lombard G. First observation on the use of oxygen under high pressure for the treatment of traumatic coma. In: Boerema, Brummelkamp, Meigne editor(s). Clinical Application of Hyperbaric Oxygen. Amsterdam: Elsevier, 1964:168‐73.
Fearnside 1997
-
- Fearnside MR, Gurka JA. The challenge of traumatic brain injury. Medical Journal of Australia 1997;167(6):293‐4. [MEDLINE: ] - PubMed
Fiskum 2000
-
- Fiskum G. Mitochondrial participation in ischemic and traumatic neural cell death. Journal of Neurotrauma 2000;17(10):843‐55. - PubMed
Hayakawa 1971
Higgins 2011 [Computer program]
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011].. The Cochrane Collaboration. The Cochrane Collaboration, 2011.
Hills 1999
-
- Hills BA. A role of oxygen‐induced osmosis in hyperbaric oxygen therapy. Medical Hypotheses 1999;52(3):259‐63. - PubMed
Holbach 1977
-
- Holbach KH, Caroli A, Wassmann H. Cerebral energy metabolism in patients with brain lesions of normo‐ and hyperbaric oxygen pressures. Journal of Neurology 1977;217(1):17‐30. [MEDLINE: ] - PubMed
Ikeda 1990
-
- Ikeda Y, Long DM. The molecular basis of brain injury and brain edema: the role of oxygen free radicals. Neurosurgery 1990;27(1):1‐11. - PubMed
Jouvet 1960
-
- Jouvet DJ. Semiological study of persistent troubles with the conscience. The physiopathological bases. [Etudes semiologiques des troubles prolonges de la conscience. Ses bases physiopathologiques]. Lyon Medecine 1960;201:1401‐20.
Khan 2003
-
- Khan B, Evans AW, Easterbrook M. Refractive changes in patients undergoing hyperbaric oxygen therapy: a prospective study. Undersea and Hyperbaric Medicine 2003;24 Suppl:9.
Langham 2005
-
- Langham J, Goldfrad C, Teasdale G, Shaw D, Rowan K. Calcium channel blockers for acute traumatic brain injury. Cochrane Database of Systematic Reviews 2005, Issue 4. [DOI: 10.1002/14651858.CD000565] - DOI
Leibson 2011
McDonagh 2004
-
- McDonagh M, Helfand M, Carson S, Russman BS. Hyperbaric oxygen therapy for traumatic brain injury: a systematic review of the evidence. Archives of Physical Medicine and Rehabilitation 2004;85(7):1198‐204. - PubMed
Meyer 2010
-
- Meyer MJ, Megyesi J, Meythaler J, Murie‐Fernandez M, Aubut JA, Foley N, Salter K, Bayley M, Marshall S, Teasell R. Acute management of acquired brain injury part I: an evidence‐based review of non‐pharmacological interventions. Brain Injury 2010;24(5):694‐705. - PubMed
Muizelaar 1989
-
- Muizelaar JP. Cerebral blood flow, cerebral blood volume and cerebral metabolism after severe head injury. In: Becker DP, Gudeman SK editor(s). Textbook of Head Injury. Philadelphia: WB Saunders, 1989:221‐40.
Murray 1999
-
- Murray GD, Teasdale GM, Braakman R, Cohadon F, Dearden M, Iannotti F, Karimi A, Lapierre F, Maas A, Ohman J, Persson L, Servadei F, Stocchetti N, Trojanowski T, Unterberg A. The European Brain Injury Consortium survey of head injuries. Acta Neurochirurgica 1999;141:223‐6. - PubMed
Neubauer 1994
-
- Neubauer RA, Gottlieb SF, Pevsner NH. Hyperbaric oxygen for treatment of closed head injury. Southern Medical Journal 1994;87(9):933‐6. - PubMed
RevMan [Computer program]
-
- The Nordic Cochrane Centre. Review Manager (RevMan). Version 5.1. Copenhagen: The Cochrane Collaboration, 2011.
Roberts 1995
Roberts 2009
Roberts 2012
Robertson 1989
-
- Robertson CS, Narayan RK, Gokaslan ZL, Pahwa R, Grossman RG, Caram P Jr, et al. Cerebral arteriovenous oxygen difference as an estimate of cerebral blood flow in comatose patients. Journal of Neurosurgery 1989;70(2):222‐30. [MEDLINE: ] - PubMed
Rockswold 2007
-
- Rockswold SB, Rockswold GL, Defillo A. Hyperbaric oxygen in traumatic brain injury. Neurology Research 2007;29(2):162‐72. - PubMed
Schierhout 2003
Siesjo 1989
-
- Siesjo BK, Agardh CD, Bengtsson F. Free radicals and brain damage. Cerebrovascular and Brain Metabolism Review 1989;1:165‐211. [MEDLINE: ] - PubMed
Stein 2010
-
- Stein SC, Georgoff P, Meghan S, Mizra K, Sonnad SS. 150 years of treating severe traumatic brain injury: a systematic review of progress in mortality. Journal of Neurotrauma 2010;27:1343–53. - PubMed
Steiner 2006
-
- Steiner LA, Andrews PJ. Monitoring the injured brain: ICP and CBF. British Journal of Anaesthesia 2006;97(1):26‐38. [DOI: ] - PubMed
Sukoff 1982
-
- Sukoff MH, Ragatz RE. Hyperbaric oxygenation for the treatment of acute cerebral edema. Neurosurgery 1982;10(1):29‐38. - PubMed
Sydenham 2009
Thurman 1999
-
- Thurman DJ, Alverson C, Browne D, et al. Traumatic brain injury in the United States: a report to congress. US Department of health and Human Services, National Centre for Injury Prevention and Control 1999.
Tymianski 1996
-
- Tymianski M, Tator CH. Normal and abnormal calcium homeostasis in neurons: a basis for the pathophysiology of traumatic and ischemic central nervous system injury. Neurosurgery 1996;38(6):1176‐95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials