

Proximal renal tubular acidosis: a not so rare disorder of multiple etiologies
- PMID: 23235953
- PMCID: PMC3616759
- DOI: 10.1093/ndt/gfs493
Proximal renal tubular acidosis: a not so rare disorder of multiple etiologies
Abstract
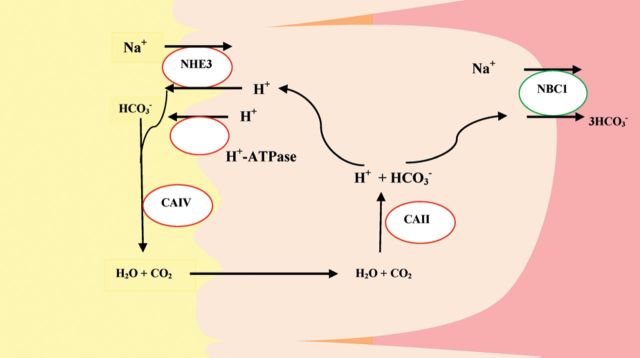
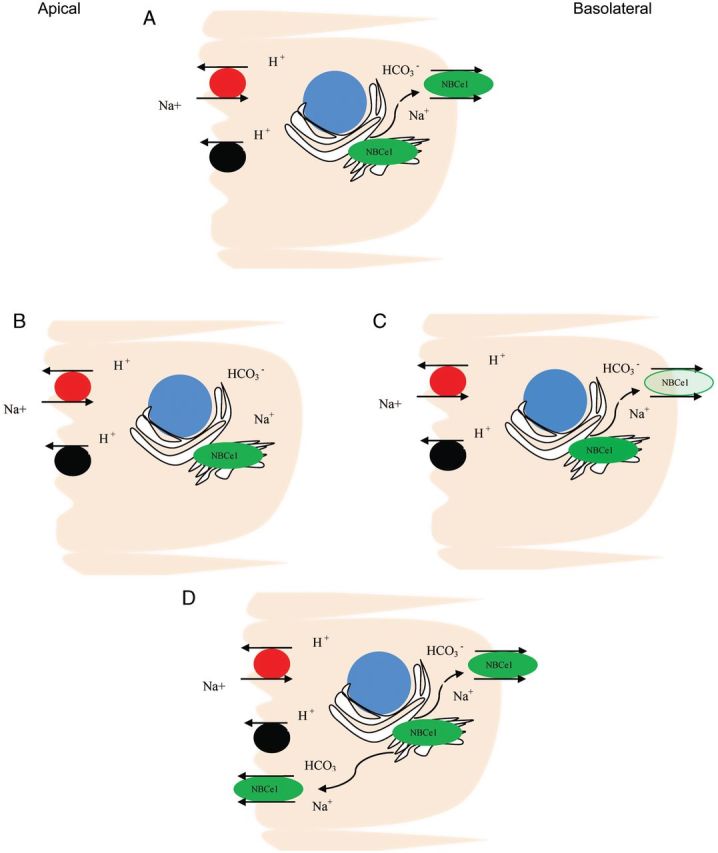
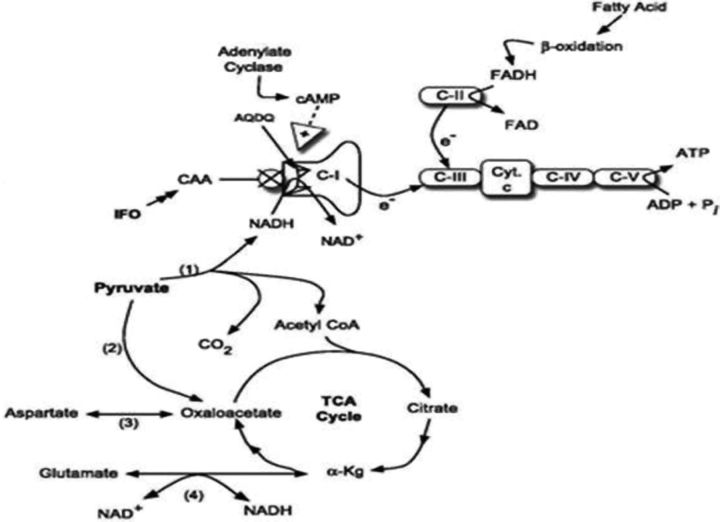
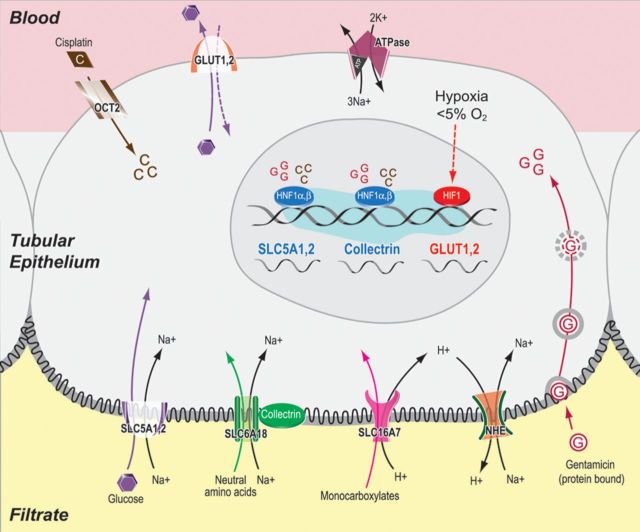
Proximal renal tubular acidosis (RTA) (Type II RTA) is characterized by a defect in the ability to reabsorb HCO(3) in the proximal tubule. This is usually manifested as bicarbonate wastage in the urine reflecting that the defect in proximal tubular transport is severe enough that the capacity for bicarbonate reabsorption in the thick ascending limb of Henle's loop and more distal nephron segments is overwhelmed. More subtle defects in proximal bicarbonate transport likely go clinically unrecognized owing to compensatory reabsorption of bicarbonate distally. Inherited proximal RTA is more commonly autosomal recessive and has been associated with mutations in the basolateral sodium-bicarbonate cotransporter (NBCe1). Mutations in this transporter lead to reduced activity and/or trafficking, thus disrupting the normal bicarbonate reabsorption process of the proximal tubules. As an isolated defect for bicarbonate transport, proximal RTA is rare and is more often associated with the Fanconi syndrome characterized by urinary wastage of solutes like phosphate, uric acid, glucose, amino acids, low-molecular-weight proteins as well as bicarbonate. A vast array of rare tubular disorders may cause proximal RTA but most commonly it is induced by drugs. With the exception of carbonic anhydrase inhibitors which cause isolated proximal RTA, drug-induced proximal RTA is associated with Fanconi syndrome. Drugs that have been recently recognized to cause severe proximal RTA with Fanconi syndrome include ifosfamide, valproic acid and various antiretrovirals such as Tenofovir particularly when given to human immunodeficiency virus patients receiving concomitantly protease inhibitors such as ritonavir or reverse transcriptase inhibitors such as didanosine.
Figures
References
-
- Moorthi K, Batlle D. Renal Tubular Acidosis. In: Gennari J, Adrogue HJ, Galla JH, Madias NE, editors. Acid–Base Disorders and Their Treatment. Boca Raton: Taylor and Francis; 2005. pp. 417–459.
-
- Katzir Z, Dinour D, Reznik-Wolf H, Nissenkorn A, Holtzman E. Familial pure proximal renal tubular acidosis–a clinical and genetic study. Nephrol Dial Transplant. 2008;23:1211–1215. doi:10.1093/ndt/gfm583. - DOI - PubMed
-
- Demirci FY, Chang MH, Mah TS, Romero MF, Gorin MB. Proximal renal tubular acidosis and ocular pathology: a novel missense mutation in the gene (SLC4A4) for sodium bicarbonate cotransporter protein (NBCe1) Mol Vis. 2006;12:324–330. - PubMed
-
- Dinour D, Chang MH, Satoh J, et al. A novel missense mutation in the sodium bicarbonate cotransporter (NBCe1/SLC4A4) causes proximal tubular acidosis and glaucoma through ion transport defects. J Biol Chem. 2004;279:52238–52246. doi:10.1074/jbc.M406591200. - DOI - PubMed
-
- Igarashi T, Inatomi J, Sekine T, et al. Mutations in SLC4A4 cause permanent isolated proximal renal tubular acidosis with ocular abnormalities. Nat Genet. 1999;23:264–266. doi:10.1038/15440. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
