

The incidence and pattern of coronary artery anomalies in the north-west of iran: a coronary arteriographic study
- PMID: 23236327
- PMCID: PMC3518709
- DOI: 10.4070/kcj.2012.42.11.753
The incidence and pattern of coronary artery anomalies in the north-west of iran: a coronary arteriographic study
Abstract
Background and objectives: Coronary artery anomalies are found in approximately 1% of patients undergoing diagnostic coronary angiography (CAG). Angiographic recognition of these vessels is important because of their clinical significance and importance in patients undergoing coronary angioplasty or cardiac surgery. There are fairly enough reports concerning the incidence of coronary anomalies in different geographic areas, but this is the first study among the Iranian population.
Subjects and methods: We reviewed the database of the Catheterization Laboratory of Imam Reza and Shahid Madani Hospitals, Tabriz University of Medical Sciences, Iran. Our inquiry included all patients who referred for CAG from other hospitals, between February 2007 and April 2009. Patients with congenital heart diseases, high "take off" of coronary arteries and separate origin of the conus artery from the right coronary sinus (RCS) were excluded. In total, 6065 films were reviewed.
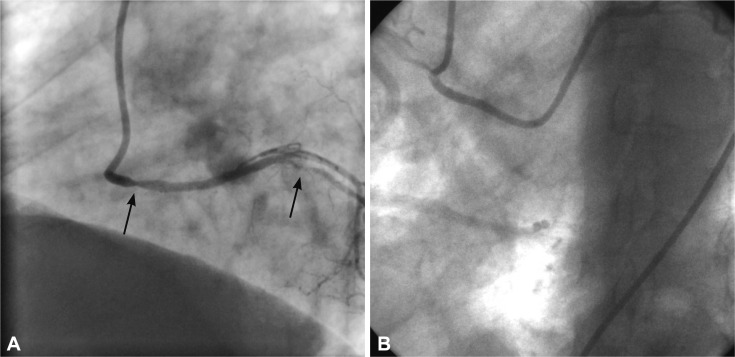
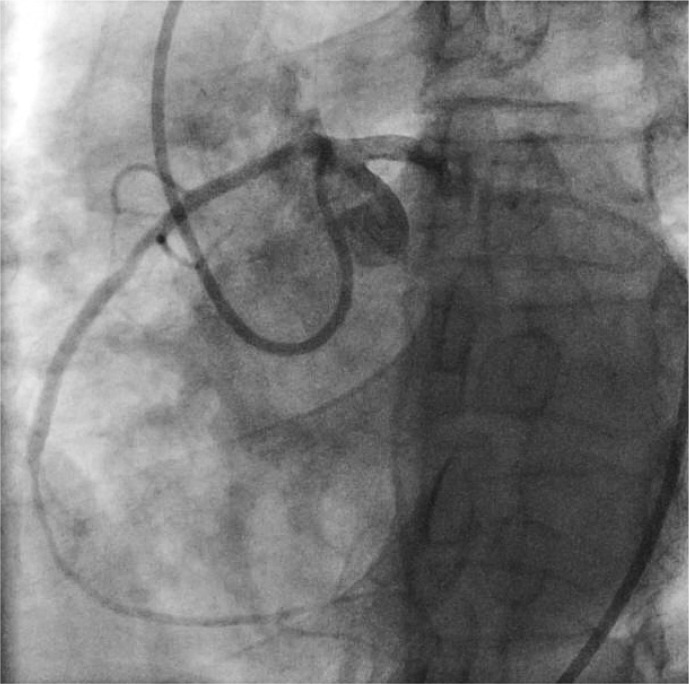
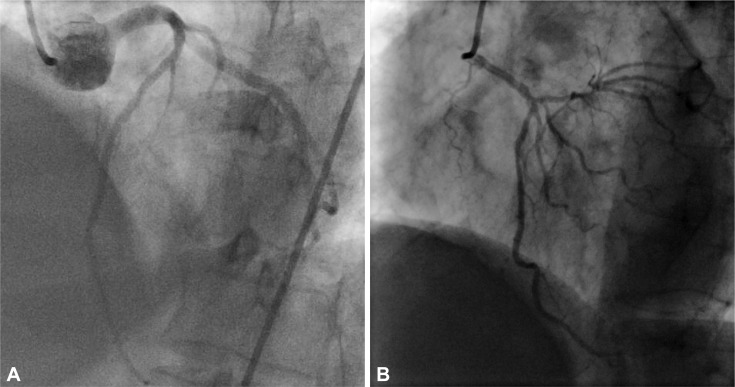
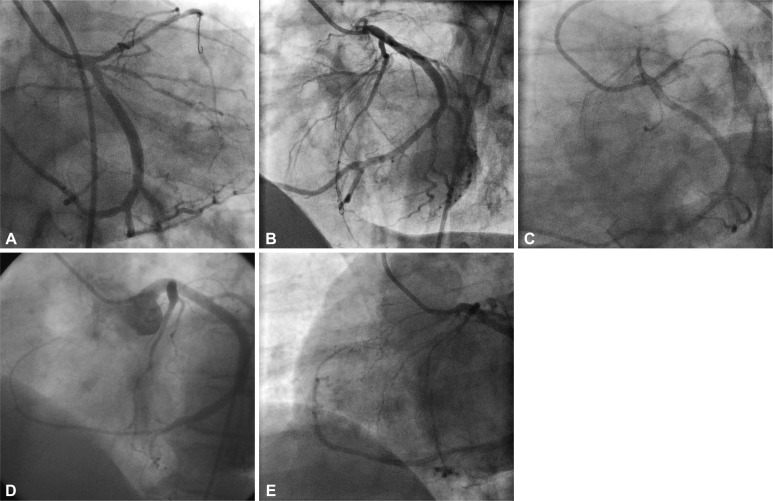
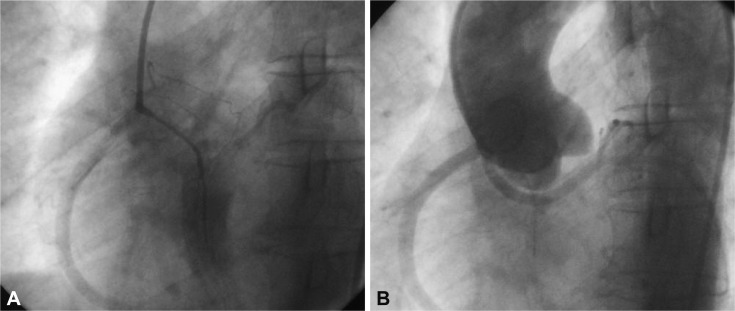
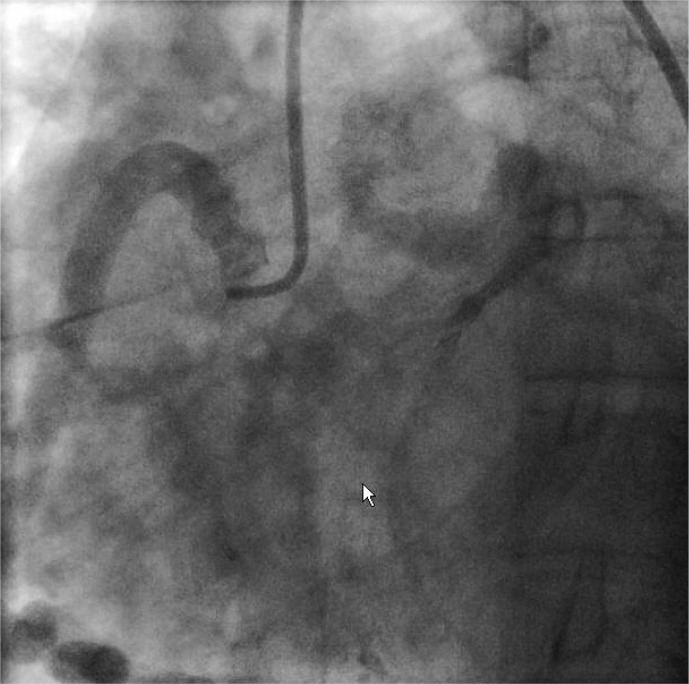
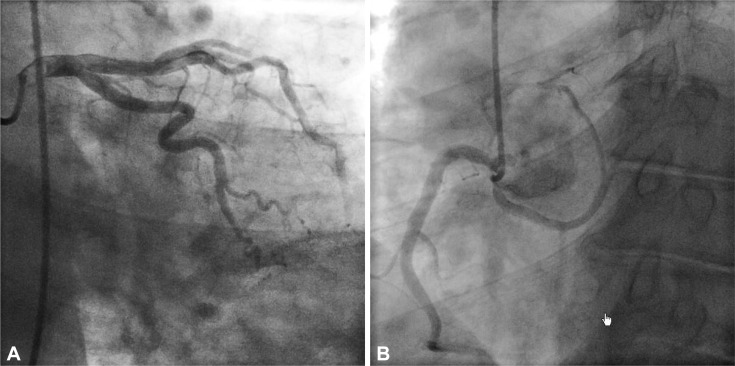
Results: Seventy nine (1.30%) patients were found to have coronary anomalies. Seventy five (1.24%) patients had anomalies of origin and distribution, while four (0.06%) had coronary artery fistulae. Most common anomaly was separate ostia of the left anterior descending artery and left circumflex artery, which was found in 42 patients (53.16%) with angiographic incidence of 0.69%. The next most common anomalies were anomalous circumflex artery from RCS/right coronary artery (RCA) {n=17 (21.51%)}, and anomalous RCA arising from left coronary sinus {n=6 (7.59%)}.
Conclusion: In general, the incidence and pattern of coronary anomalies in our study was similar to earlier reports from different parts of the world.
Keywords: Accept; Angiography; Coronary arteries.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures

References
-
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28–40. - PubMed
-
- Cieslinski G, Rapprich B, Kober G. Coronary anomalies: incidence and importance. Clin Cardiol. 1993;16:711–715. - PubMed
-
- Cheitlin MD, De Castro CM, McAllister HA. Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva, A not-so-minor congenital anomaly. Circulation. 1974;50:780–787. - PubMed
-
- Chaitman BR, Lespérance J, Saltiel J, Bourassa MG. Clinical, angiographic, and hemodynamic findings in patients with anomalous origin of the coronary arteries. Circulation. 1976;53:122–131. - PubMed
-
- Kragel AH, Roberts WC. Anomalous origin of either the right or left main coronary artery from the aorta with subsequent coursing between aorta and pulmonary trunk: analysis of 32 necropsy cases. Am J Cardiol. 1988;62(10 Pt 1):771–777. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
