

When does overuse of antibiotics become a tragedy of the commons?
- PMID: 23236344
- PMCID: PMC3517551
- DOI: 10.1371/journal.pone.0046505
When does overuse of antibiotics become a tragedy of the commons?
Abstract
Background: Over-prescribing of antibiotics is considered to result in increased morbidity and mortality from drug-resistant organisms. A resulting common wisdom is that it would be better for society if physicians would restrain their prescription of antibiotics. In this view, self-interest and societal interest are at odds, making antibiotic use a classic "tragedy of the commons".
Methods and findings: We developed two mathematical models of transmission of antibiotic resistance, featuring de novo development of resistance and transmission of resistant organisms. We analyzed the decision to prescribe antibiotics as a mathematical game, by analyzing individual incentives and community outcomes.
Conclusions: A conflict of interest may indeed result, though not in all cases. Increased use of antibiotics by individuals benefits society under certain circumstances, despite the amplification of drug-resistant strains or organisms. In situations where increased use of antibiotics leads to less favorable outcomes for society, antibiotics may be harmful for the individual as well. For other scenarios, where a conflict between self-interest and society exists, restricting antibody use would benefit society. Thus, a case-by-case assessment of appropriate use of antibiotics may be warranted.
Conflict of interest statement
Figures
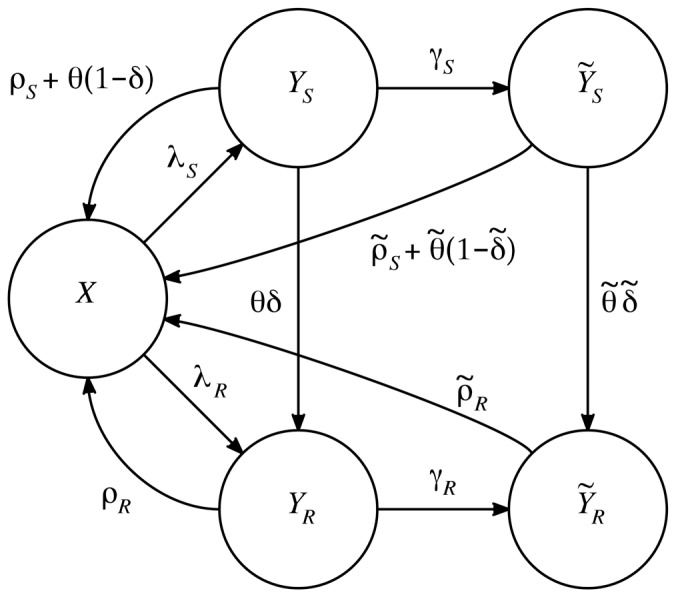
 —the number of uninfected individuals,
—the number of uninfected individuals,  —the number of individuals with mild infection by the drug-sensitive organism,
—the number of individuals with mild infection by the drug-sensitive organism,  —the number of individuals with severe infection by the drug-sensitive organism,
—the number of individuals with severe infection by the drug-sensitive organism,  —the number of individuals with mild infection by the drug-resistant organism, and
—the number of individuals with mild infection by the drug-resistant organism, and  —the number of individuals with severe infection by the drug-resistant organism. Treatment rates for the mild and severe state are given by
—the number of individuals with severe infection by the drug-resistant organism. Treatment rates for the mild and severe state are given by  and
and  , respectively. The arrows are labeled with per-individual flow rates; the total flow rate from each state along each arrow is given by the label of the arrow times the number of individuals in the state. The explicit differential equations and parameter definitions are given in the main text.
, respectively. The arrows are labeled with per-individual flow rates; the total flow rate from each state along each arrow is given by the label of the arrow times the number of individuals in the state. The explicit differential equations and parameter definitions are given in the main text.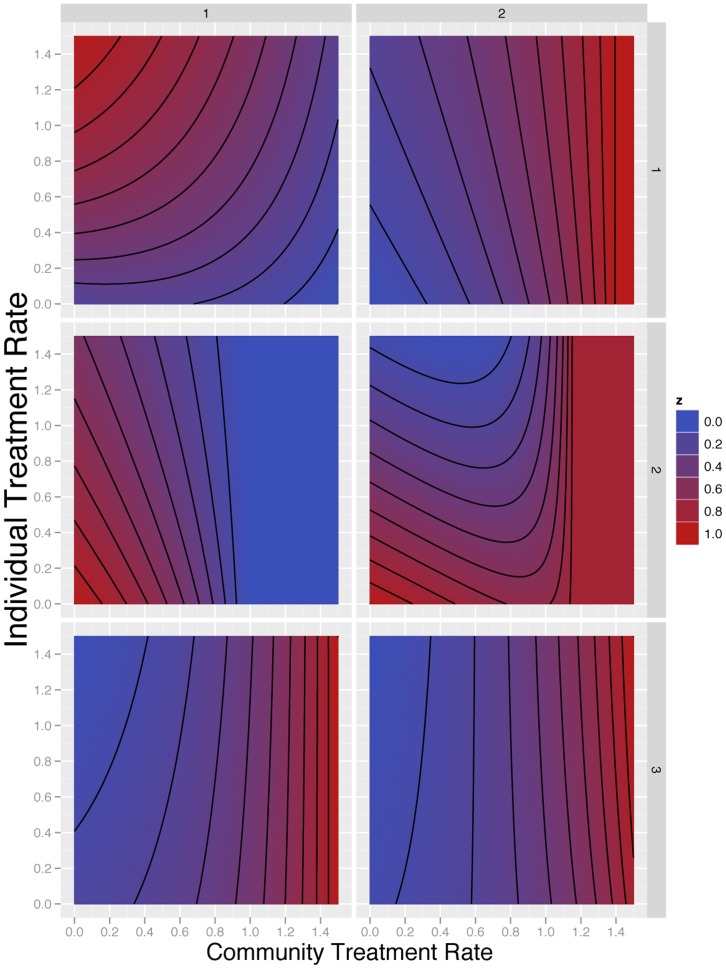
 -axes are the community level of treatment, i.e. the strategy assumed chosen by all other members of the community. The
-axes are the community level of treatment, i.e. the strategy assumed chosen by all other members of the community. The  -axes are the level of treatment chosen by an individual within the community. The contour plot shows the fraction of time spent by this person, in the severe state; each panel has been scaled so that the minimum value is zero (blue) and the maximum value is 1 (red). The numerical parameter choices are given in Table 2, and the minimum and maximum values for each panel.
-axes are the level of treatment chosen by an individual within the community. The contour plot shows the fraction of time spent by this person, in the severe state; each panel has been scaled so that the minimum value is zero (blue) and the maximum value is 1 (red). The numerical parameter choices are given in Table 2, and the minimum and maximum values for each panel.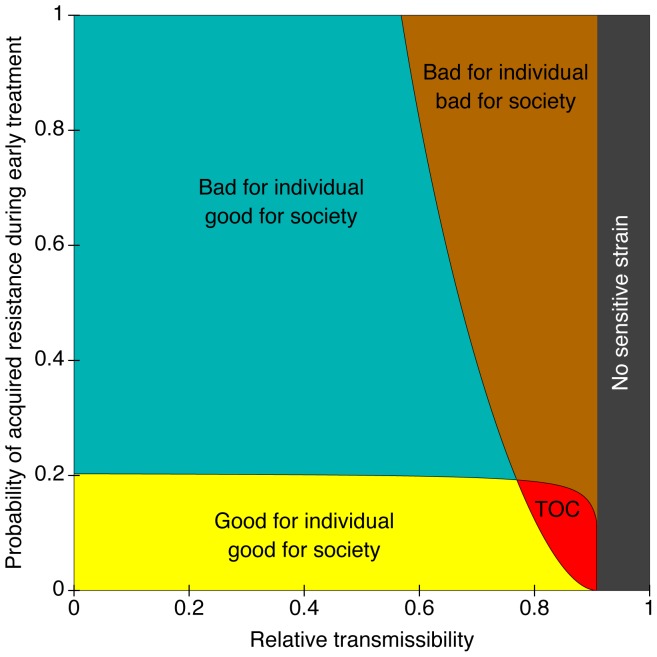
 ,
,  ,
,  ,
,  ,
,  ,
,  , and
, and  . The horizontal axis corresponds to
. The horizontal axis corresponds to  and the vertical axis to
and the vertical axis to  .
.References
-
- Travis J (1994) Reviving the antibiotic miracle? Science 264: 360–362. - PubMed
-
- Cohen ML (1992) Epidemiology of drug resistance: implications for a post-antimicrobial era. Science 257: 1050–1055. - PubMed
-
- Neu HC (1992) The crisis in antibiotic resistance. Science 257: 1064–1073. - PubMed
-
- Levy SB, Marshall B (2004) Antibacterial resistance worldwide: causes, challenges and responses. Nature, Medicine 10: S122–S129. - PubMed
-
- Hardin G (1968) The tragedy of the commons. Science 162: 1243–1248. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
