

Endomyocardial biopsy for monitoring heart transplant patients: 11-years-experience at a german heart center
- PMID: 23236543
- PMCID: PMC3515982
Endomyocardial biopsy for monitoring heart transplant patients: 11-years-experience at a german heart center
Abstract
Background: Heart transplantation (HTX) has become an established therapy for patients with end-stage heart failure. Endomyocardial biopsy (EMB) still represents the gold standard for routine surveillance of heart transplant rejection. The objective of this article is to report our experience regarding the use of EMB in monitoring heart transplant recipients.
Methods: We evaluated retrospectively all patients who underwent orthotopic HTX between 2000 and 2011 at our hospital. From all patients, we created a follow-up, determined the number of EMB events and described the complications associated with this procedure.
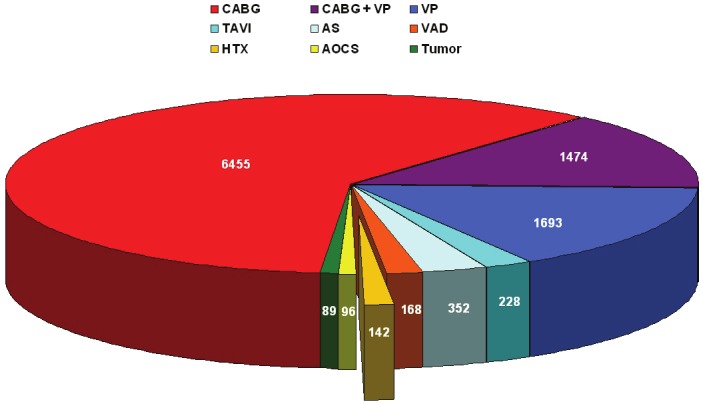
Results: HTX was performed in 142 cases at our center in the last 11 years (1.3% of the total of 10693 cardiac surgical operations in that period). Further 9 patients visited our department for monitoring after HTX performed at an external center (total: 151). For all patients, a total of 1896 EMB events have been recorded. The majority of biopsies were performed through the right internal jugular vein. The overall complication rate was 1% (n=19).
Conclusions: The histological examination of right ventricular EMB still represents the gold standard of care for cardiac allograft rejection monitoring. EMB is an invasive, but safe and dedicated diagnostic procedure. However, the usefulness of recent non-invasive diagnostic approaches as an adjunct tool in monitoring for rejection remains to be further analyzed.
Keywords: Endomyocardial biopsy; allograft rejection; cardiac transplantation; histopathological evaluation; immunosuppression.
Figures
Similar articles
-
Endomyocardial biopsy via the femoral access - still safe and valuable diagnostic tool.BMC Cardiovasc Disord. 2016 Nov 15;16(1):222. doi: 10.1186/s12872-016-0406-0. BMC Cardiovasc Disord. 2016. PMID: 27846815 Free PMC article.
-
Endomyocardial biopsy in pediatric heart transplant recipients: a useful exercise? (Analysis of 1,169 biopsies).Pediatr Transplant. 2000 Aug;4(3):186-92. doi: 10.1034/j.1399-3046.2000.00100.x. Pediatr Transplant. 2000. PMID: 10933318
-
Tricuspid valve injury after heart transplantation due to endomyocardial biopsy: an analysis of 3550 biopsies.Transplant Proc. 2012 Oct;44(8):2479-82. doi: 10.1016/j.transproceed.2012.07.024. Transplant Proc. 2012. PMID: 23026624
-
Heart transplant biopsies: interpretation and significance.J Clin Pathol. 2010 Jan;63(1):12-20. doi: 10.1136/jcp.2009.072462. Epub 2009 Oct 26. J Clin Pathol. 2010. PMID: 19858528 Review.
-
An approach to endomyocardial biopsy interpretation.J Clin Pathol. 2006 Feb;59(2):121-9. doi: 10.1136/jcp.2005.026443. J Clin Pathol. 2006. PMID: 16443725 Free PMC article. Review.
Cited by
-
Revisiting transplant immunology through the lens of single-cell technologies.Semin Immunopathol. 2023 Jan;45(1):91-109. doi: 10.1007/s00281-022-00958-0. Epub 2022 Aug 18. Semin Immunopathol. 2023. PMID: 35980400 Free PMC article. Review.
-
Successful venous angioplasty of superior vena cava syndrome after heart transplantation.Case Rep Cardiol. 2014;2014:490276. doi: 10.1155/2014/490276. Epub 2014 Aug 3. Case Rep Cardiol. 2014. PMID: 25161772 Free PMC article.
-
Case report of a coronary artery-right ventricular fistula following repeat endomyocardial biopsies in a heart transplant patient.Eur Heart J Case Rep. 2021 Jun 26;5(6):ytab224. doi: 10.1093/ehjcr/ytab224. eCollection 2021 Jun. Eur Heart J Case Rep. 2021. PMID: 34189402 Free PMC article.
-
Percutaneous Closure of Ventricle Pseudoaneurysm-A Complication of Endomyocardial Biopsy in a Pediatric Heart Transplant Recipient: A Case Report.CJC Open. 2024 Oct 16;7(1):100-102. doi: 10.1016/j.cjco.2024.10.006. eCollection 2025 Jan. CJC Open. 2024. PMID: 39872655 Free PMC article. No abstract available.
-
Endomyocardial biopsy via the femoral access - still safe and valuable diagnostic tool.BMC Cardiovasc Disord. 2016 Nov 15;16(1):222. doi: 10.1186/s12872-016-0406-0. BMC Cardiovasc Disord. 2016. PMID: 27846815 Free PMC article.
References
-
- Vega JD, Moore J, Murray S, Chen JM, Johnson MR, Dyke DB. Heart transplantation in the United States, 1998-2007. Am J Transplant. 2009;9:932–41. - PubMed
-
- Patel JK, Kittleson M, Kobashigawa JA. Cardiac allograft rejection. Surgeon. 2011;9:160–7. - PubMed
-
- Boyle A. Current status of cardiac transplantation and mechanical circulatory support. Curr Heart Fail Rep. 2009;6:28–33. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical