

Reverse shoulder arthroplasty in revision of failed shoulder arthroplasty-outcome and follow-up
- PMID: 23238604
- PMCID: PMC3532649
- DOI: 10.1007/s00264-012-1742-z
Reverse shoulder arthroplasty in revision of failed shoulder arthroplasty-outcome and follow-up
Abstract
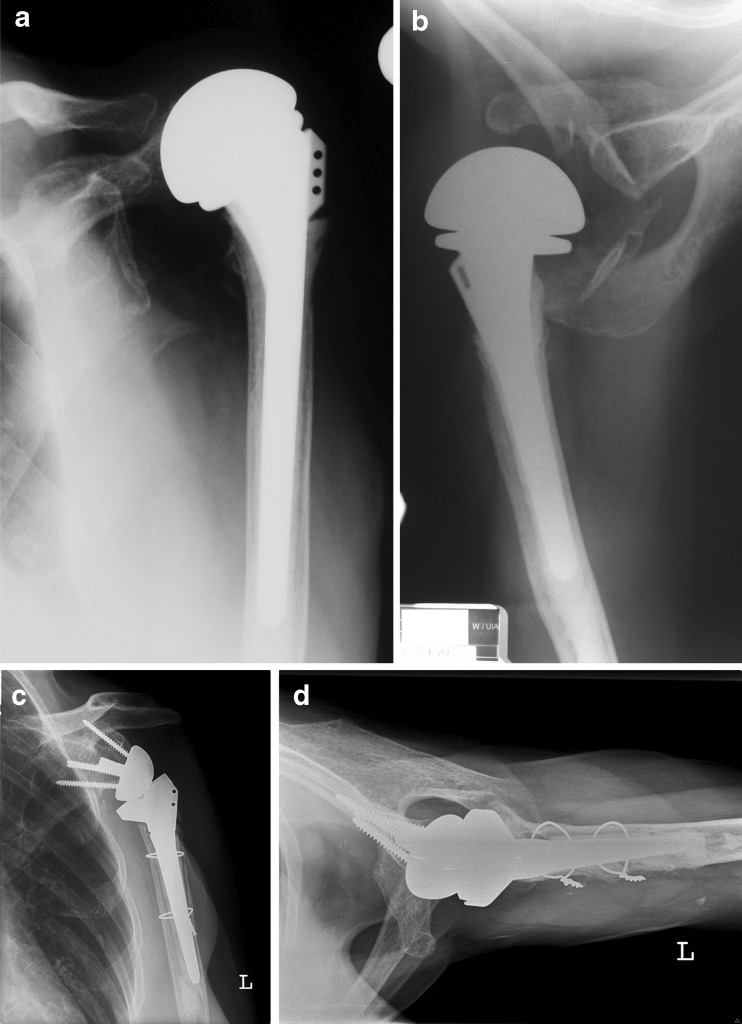
Purpose: The number of shoulder arthroplasties has increased over the last decade, which can partly be explained by the increasing use of the reverse total shoulder arthroplasty technique. However, the options for revision surgery after primary arthroplasty are limited in cases of irreparable rotator cuff deficiency, and tuberosity malunion, nonunion, or resorption. Often, conversion to a reverse design is the only suitable solution. We analysed the functional outcome, complication rate and patient satisfaction after the revision of primary shoulder arthroplasty using an inverse design.
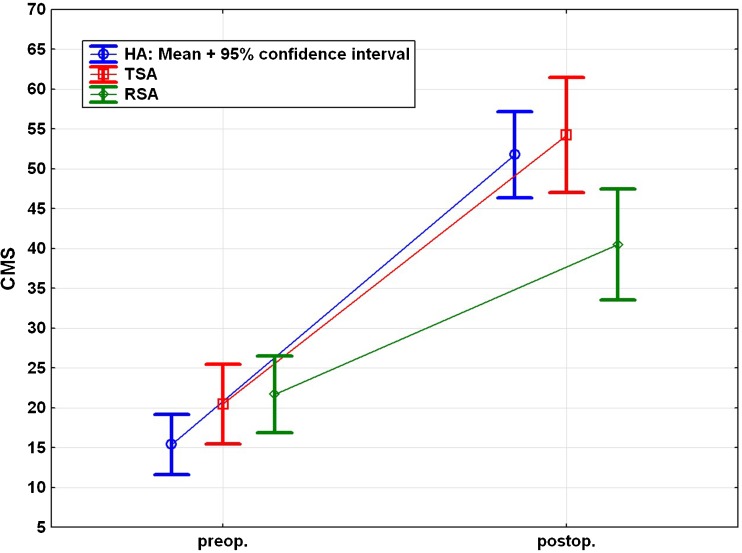
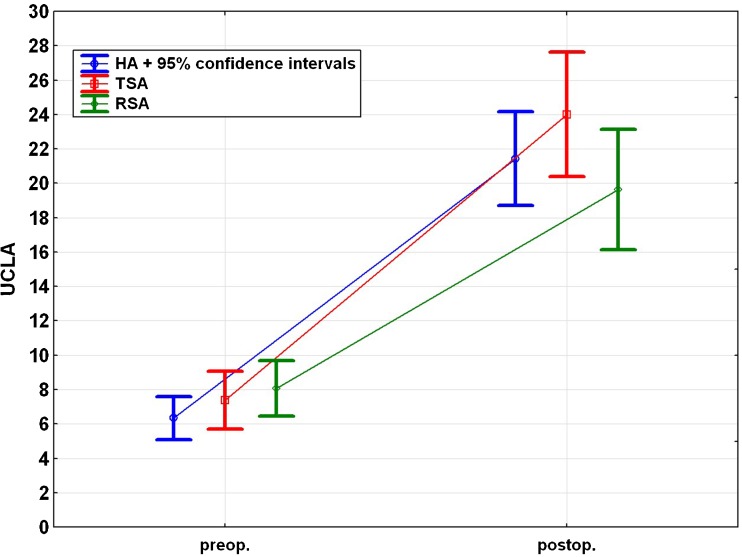
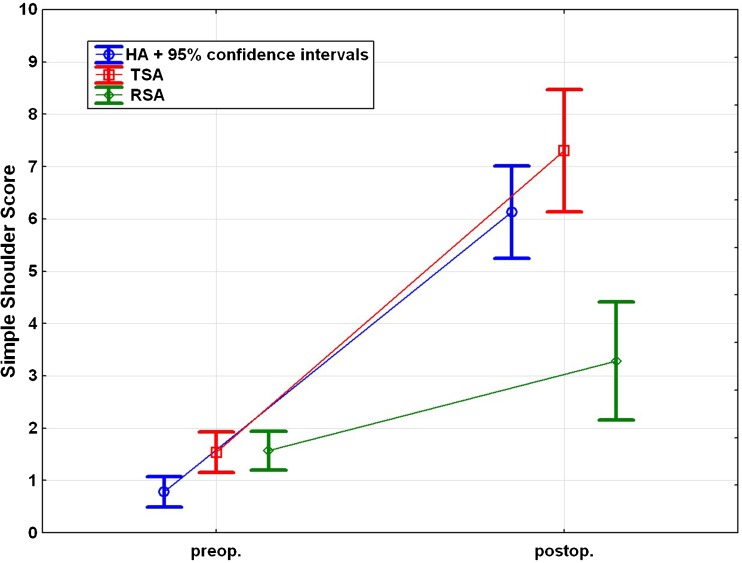
Methods: Over a ten-year period 57 patients underwent revision surgery for failed primary shoulder arthroplasty using a reverse design. Of the 57 patients, 50 (mean age, 64.2 years) were available after an average follow-up of 51 months. Clinical evaluation included the Constant Murley Score, the UCLA score, and the Simple Shoulder Test, whereas radiological evaluation included plain radiographs in standard projections. Patients were also requested to rate their subjective satisfaction of the final outcome as excellent, good, satisfied or dissatisfied.
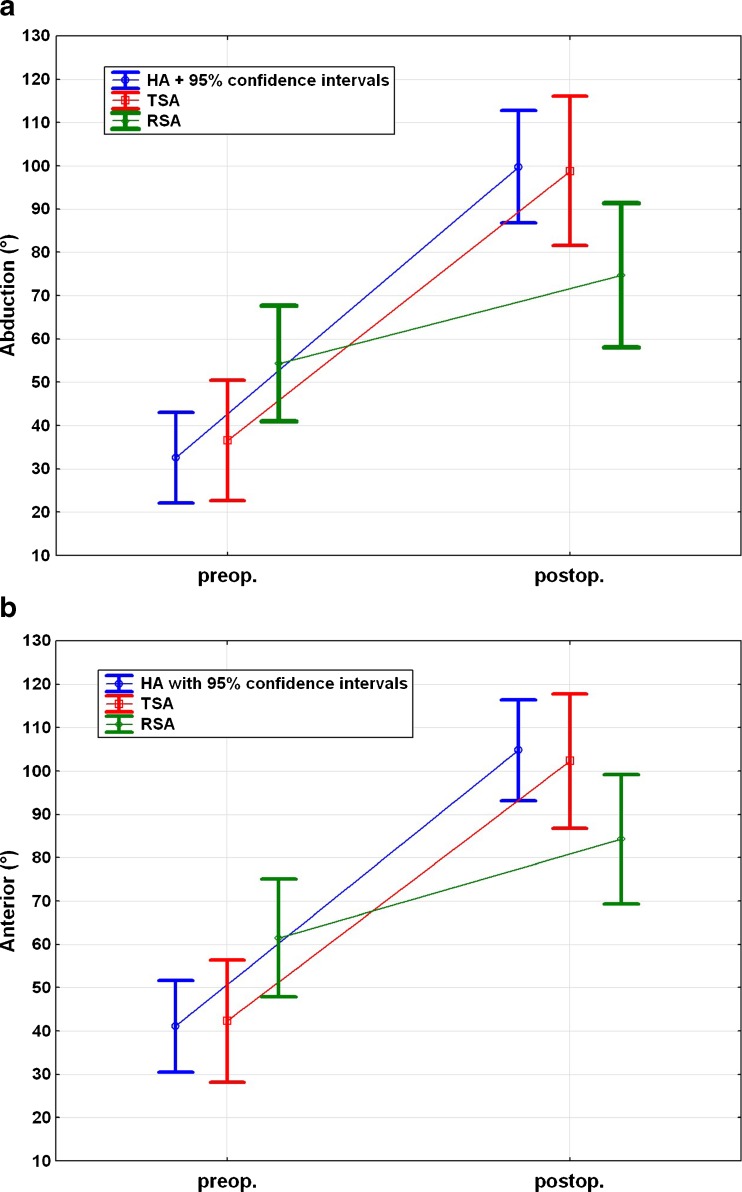
Results: Compared to the preoperative status, the overall functional outcome measurements based on standardised outcome shoulder scores improved significantly at follow-up. The overall mean Constant Murley score improved from 18.5 to 49.3 points, the mean UCLA score improved from 7.1 to 21.6 points, and the mean simple shoulder test improved from 1.2 to 5.6 points. The average degree of abduction improved from 40 to 93° (p < 0.0001), and the average degree of anterior flexion improved from 47 to 98° (p < 0.0001). The median VAS pain score decreased from 7 to 1. Complications occurred in 12 cases (24 %).A total of 32 (64 %) patients rated their result as good or excellent, six (12 %) as satisfactory and 12 (24 %) as dissatisfied.
Conclusion: In revision shoulder arthroplasty after failed primary shoulder arthroplasty an inverse design can improve the functional outcome, and patient satisfaction is usually high. However, the complication rate of this procedure is also high, and patient selection and other treatment options should be carefully considered.
Figures

References
-
- Grammont PM, Baulot E. Delta shoulder prosthesis for rotator cuff rupture. Orthopedics. 1993;16:65–68. - PubMed
-
- Barrett WP, Franklin JL, Jackins SE, Wyss CR, Matsen FA., 3rd Total shoulder arthroplasty. J Bone Joint Surg Am. 1987;69:865–872. - PubMed
-
- Arntz CT, Jackins S, Matsen FA., 3rd Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am. 1993;75:485–491. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
