

Diffusion abnormalities in pediatric mild traumatic brain injury
- PMID: 23238712
- PMCID: PMC6621719
- DOI: 10.1523/JNEUROSCI.3379-12.2012
Diffusion abnormalities in pediatric mild traumatic brain injury
Abstract
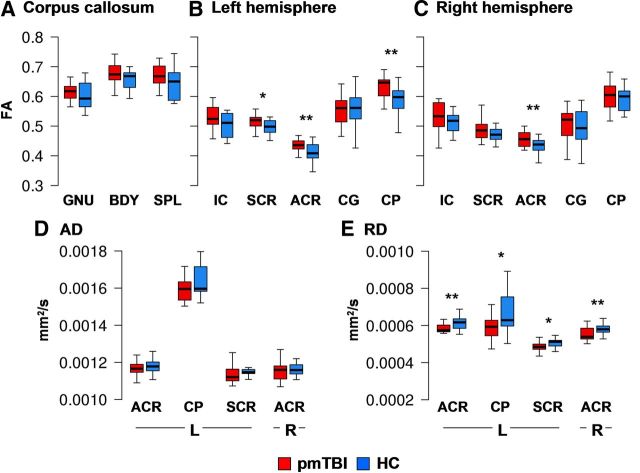
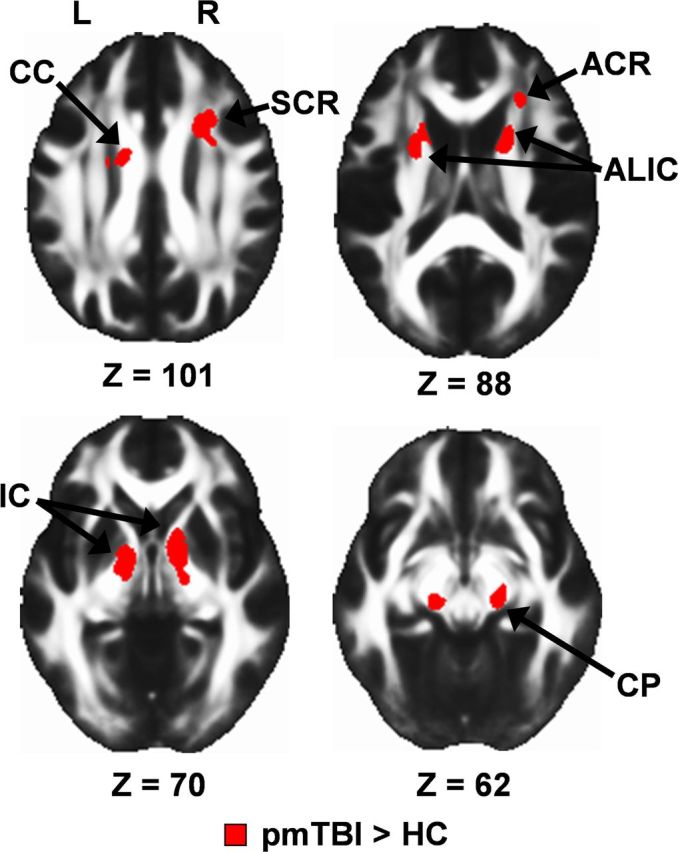
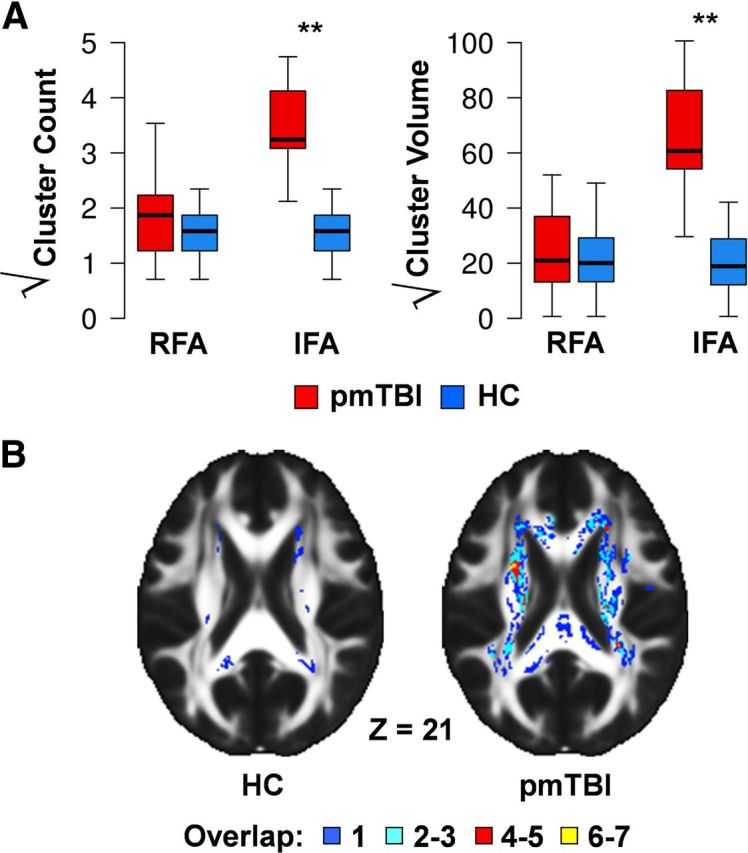
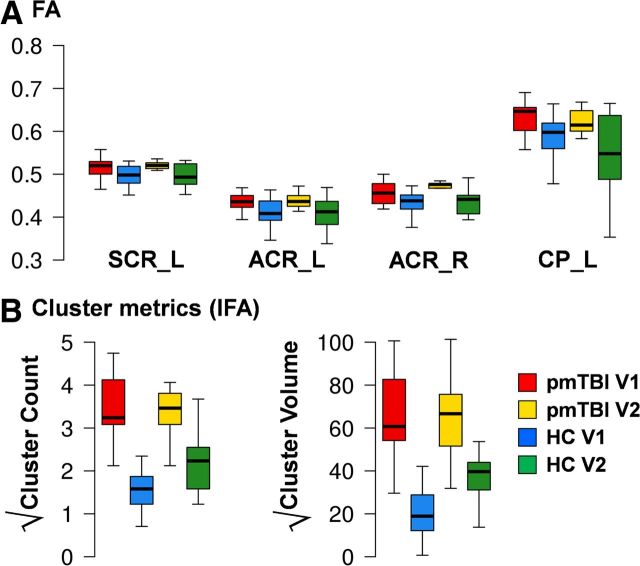
Pediatric mild traumatic brain injury (pmTBI) is the most prevalent neurological insult in children and is associated with both acute and chronic neurobehavioral sequelae. However, little is known about underlying pathophysiology and how injuries change as a function of recovery. Fractional anisotropy, axial diffusivity, and radial diffusivity were examined in 15 semi-acute pmTBI patients and 15 well-matched controls, with a subset of participants returning for a second visit. A novel analytic strategy was applied to capture spatially heterogeneous white matter injuries (lesions) in addition to standard analyses. Evidence of cognitive dysfunction after pmTBI was observed in the domains of attention (p = 0.02, d = -0.92) and processing speed (p = 0.05, d = -0.73) semi-acutely. Region of interest (ROI) and voxelwise analyses indicated increased anisotropic diffusion for pmTBI patients, with an elevated number of clusters with high anisotropy. Metrics of increased anisotropy were able to objectively classify pmTBI from healthy controls at 90% accuracy but were not associated with neuropsychological deficits. Little evidence of recovery in white matter abnormalities was observed over a 4-month interval in returning patients, indicating that physiological recovery may lag behind subjective reports of normality. Increased anisotropic diffusion has been previously linked with cytotoxic edema after TBI, and the magnitude and duration of these abnormalities appear to be greater in pediatric patients. Current findings suggest that developing white matter may be more susceptible to initial mechanical injury forces and that anisotropic diffusion provides an objective biomarker of pmTBI.
Figures
References
-
- Adelson PD, Kochanek PM. Head injury in children. J Child Neurol. 1998;13:2–15. - PubMed
-
- Akpinar E, Koroglu M, Ptak T. Diffusion tensor MR imaging in pediatric head trauma. J Comput Assist Tomogr. 2007;31:657–661. - PubMed
-
- Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Outcome from mild head injury in young children: a prospective study. J Clin Exp Neuropsychol. 2001;23:705–717. - PubMed
-
- Babikian T, Tong KA, Galloway NR, Freier-Randall MC, Obenaus A, Ashwal S. Diffusion-weighted imaging predicts cognition in pediatric brain injury. Pediatr Neurol. 2009;41:406–412. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources