

Association of large-airway lymphocytic bronchitis with bronchiolitis obliterans syndrome
- PMID: 23239157
- PMCID: PMC3603592
- DOI: 10.1164/rccm.201206-1025OC
Association of large-airway lymphocytic bronchitis with bronchiolitis obliterans syndrome
Abstract
Rationale: Lung transplantation offers great promise for otherwise terminal lung diseases, but the development of bronchiolitis obliterans syndrome (BOS) continues to limit survival. Although acute rejection and lymphocytic bronchiolitis have been identified as risk factors for the development of BOS, it is unclear whether large-airway lymphocytic inflammation conveys the same risk.
Objectives: We evaluated lymphocytic bronchitis on endobronchial biopsies as a risk factor for BOS and mortality.
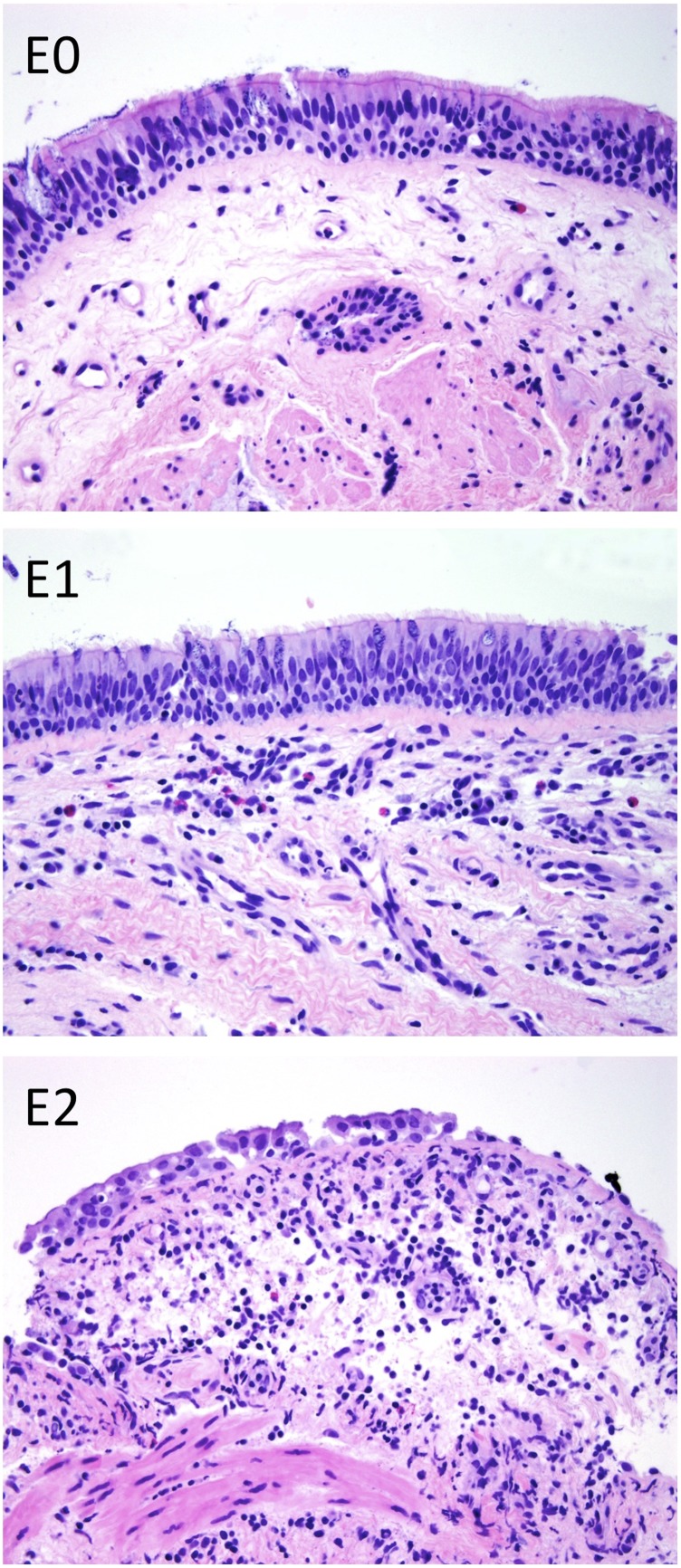
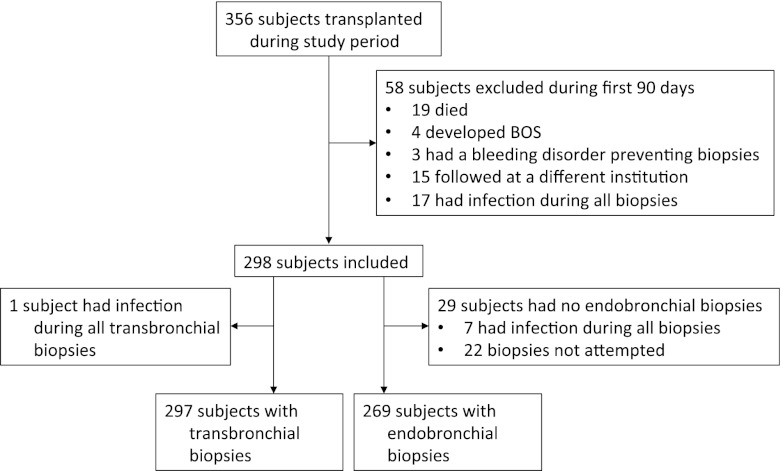
Methods: Endobronchial biopsies were collected and graded during surveillance after lung transplantation. We assessed samples with negative cultures collected in the first 90 days from 298 subjects and compared large-airway lymphocytic bronchitis assessed by a 0-2 "E-score" and with standard A and BR pathology scores for acute rejection and small-airway lymphocytic bronchiolitis, respectively.
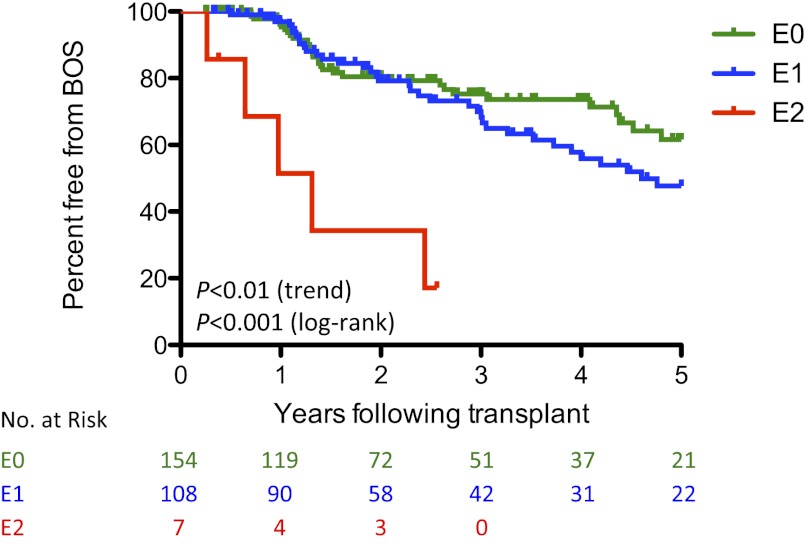
Measurements and main results: We found surprisingly little association between large- and small-airway lymphocytic inflammation scores from a given bronchoscopy. Endobronchial lymphocytic bronchitis was more prevalent in subjects in BOS stage 0p and BOS stages 1-3 at the time of biopsy. Within 90 days after transplantation, increasing maximum E-score was associated with greater risk of BOS (adjusted hazard ratio, 1.76; 95% confidence interval, 1.11-2.78; P = 0.02) and in this analysis 90-day maximum E-scores were the only score type predictive of BOS (P < 0.01).
Conclusions: These results support a multicenter study to evaluate endoscopic biopsies for the identification of patients at increased risk for BOS. The association of endobronchial lymphocytic inflammation and BOS may have mechanistic implications.
Figures
References
-
- Estenne M, Hertz MI. Bronchiolitis obliterans after human lung transplantation. Am J Respir Crit Care Med 2002;166:440–444 - PubMed
-
- Hopkins PM, McNeil K. Evidence for immunosuppression in lung transplantation. Curr Opin Organ Transplant 2008;13:477–483 - PubMed
-
- Heng D, Sharples LD, McNeil K, Stewart S, Wreghitt T, Wallwork J. Bronchiolitis obliterans syndrome: incidence, natural history, prognosis, and risk factors. J Heart Lung Transplant 1998;17:1255–1263 - PubMed
-
- Trulock EP. Management of lung transplant rejection. Chest 1993;103:1566–1576 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
