

Enhanced vestibulo-ocular reflex to electrical vestibular stimulation in Meniere's disease
- PMID: 23239162
- PMCID: PMC3540272
- DOI: 10.1007/s10162-012-0362-z
Enhanced vestibulo-ocular reflex to electrical vestibular stimulation in Meniere's disease
Abstract
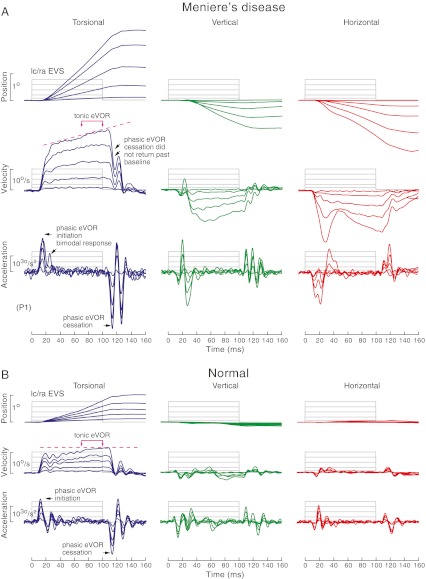
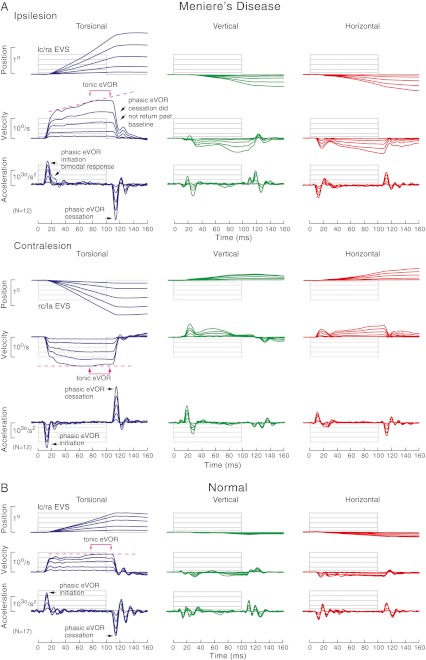
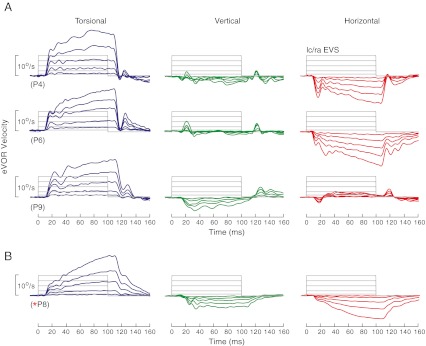
Meniere's disease is characterized by sporadic episodes of vertigo, nystagmus, fluctuating sensorineural hearing loss, tinnitus and aural pressure. Since Meniere's disease can affect different regions of the vestibular labyrinth, we investigated if electrical vestibular stimulation (EVS) which excites the entire vestibular labyrinth may be useful to reveal patchy endorgan pathology. We recorded three-dimensional electrically evoked vestibulo-ocular reflex (eVOR) to transient EVS using bilateral, bipolar 100-ms current steps at intensities of 0.9, 2.5, 5.0, 7.5 and 10.0 mA with dual-search coils in 12 unilateral Meniere's patients. Their results were compared to 17 normal subjects. Normal eVOR had tonic and phasic spatiotemporal properties best described by the torsional component, which was four times larger than horizontal and vertical components. At EVS onset and offset of 8.9 ms latency, there were phasic eVOR initiation (M = 1,267 °/s(2)) and cessation (M = -1,675 °/s(2)) acceleration pulses, whereas during the constant portion of the EVS, there was a maintained tonic eVOR (M = 9.1 °/s) at 10 mA. However in Meniere's disease, whilst latency of EVS onset and offset was normal at 9.0 ms, phasic eVOR initiation (M = 1,720 °/s(2)) and cessation (M = -2,523 °/s(2)) were enlarged at 10 mA. The initiation profile was a bimodal response, whilst the cessation profile frequently did not return to baseline. The tonic eVOR (M = 20.5 °/s) exhibited a ramped enhancement of about twice normal at 10 mA. Tonic eVOR enhancement was present for EVS >0.9 mA and disproportionately enhanced the torsional, vertical and horizontal components. These eVOR abnormalities may be a diagnostic indicator of Meniere's disease and may explain the vertigo attacks in the presence of declining mechanically evoked vestibular responses.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
