

Physiologic changes in a nonhuman primate model of HIV-associated pulmonary arterial hypertension
- PMID: 23239493
- PMCID: PMC3604086
- DOI: 10.1165/rcmb.2011-0434OC
Physiologic changes in a nonhuman primate model of HIV-associated pulmonary arterial hypertension
Abstract
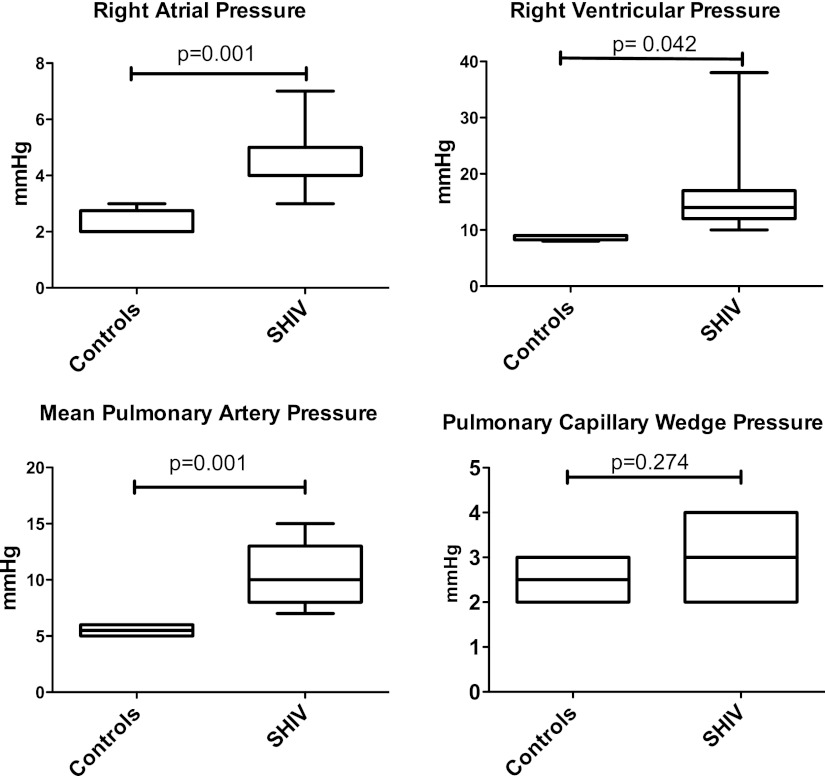
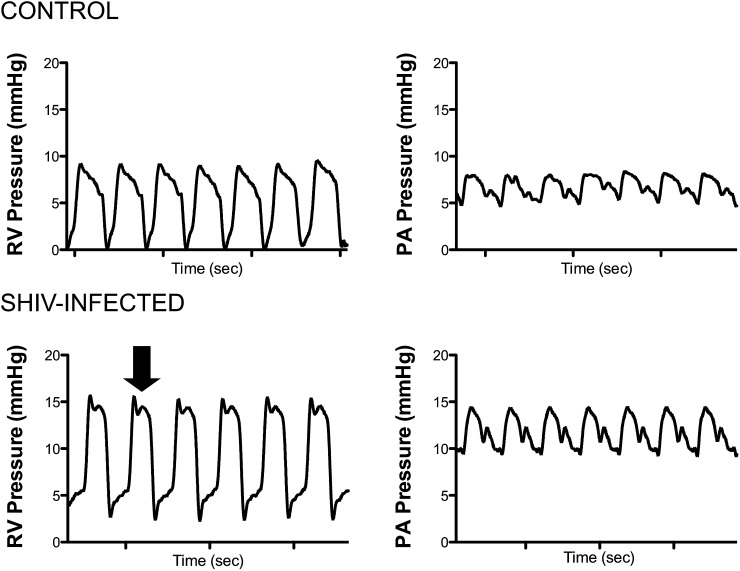
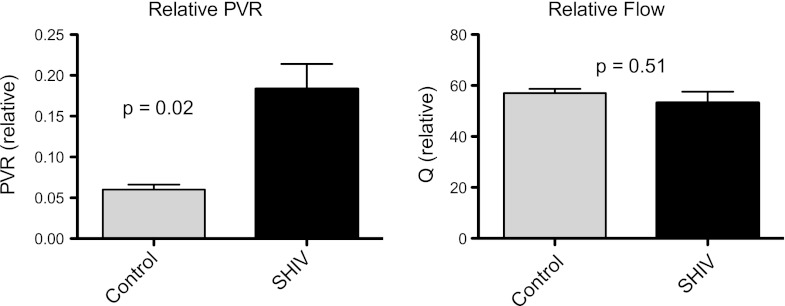
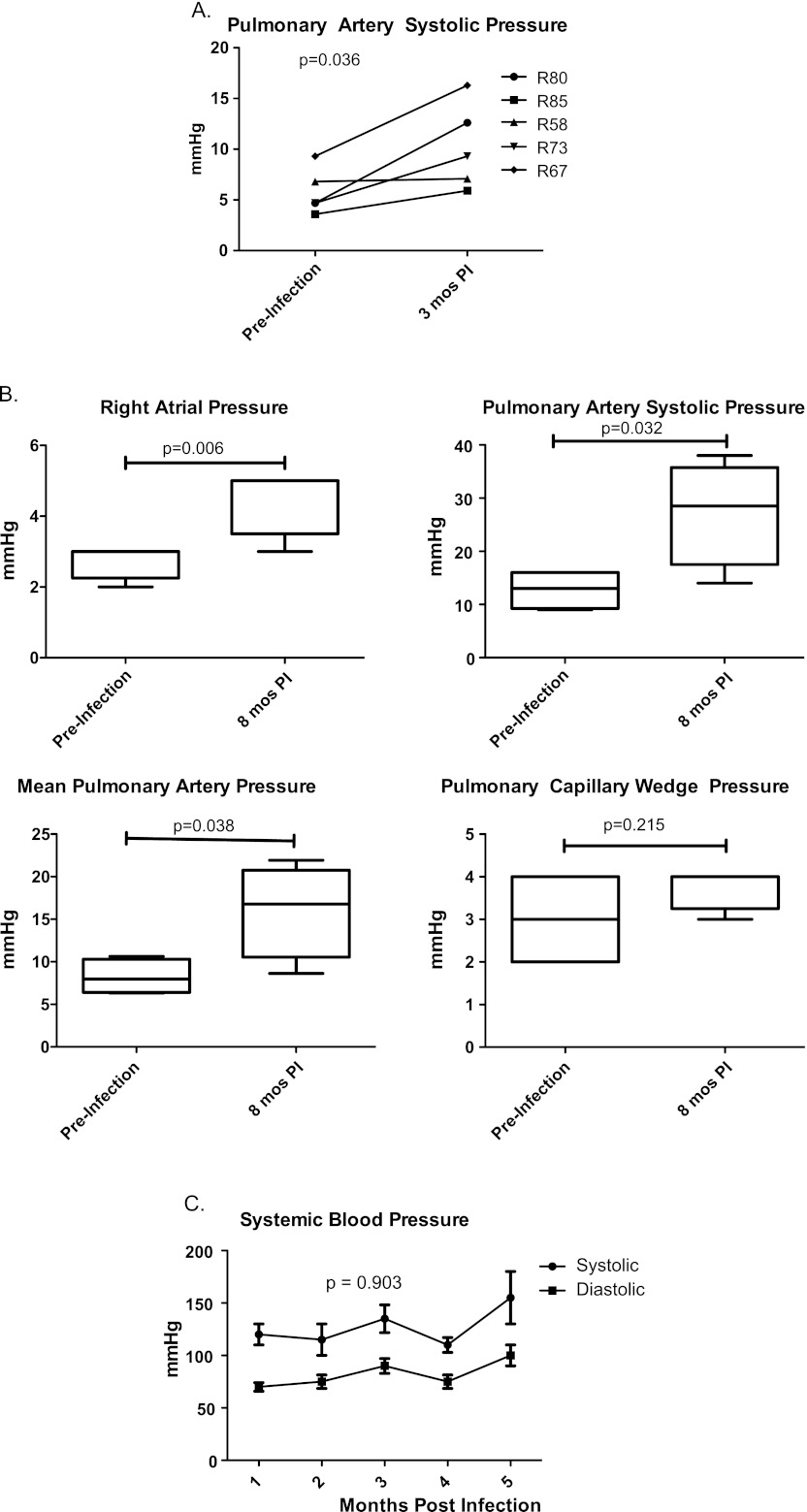
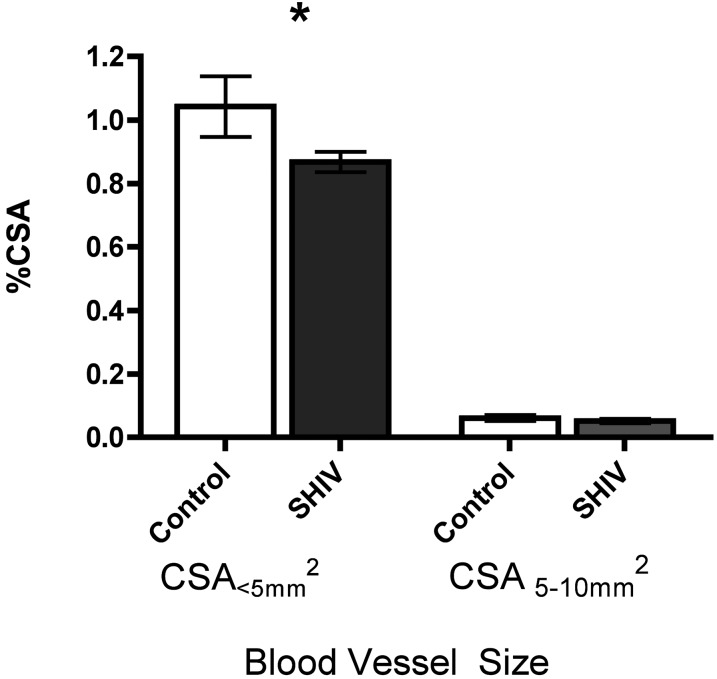
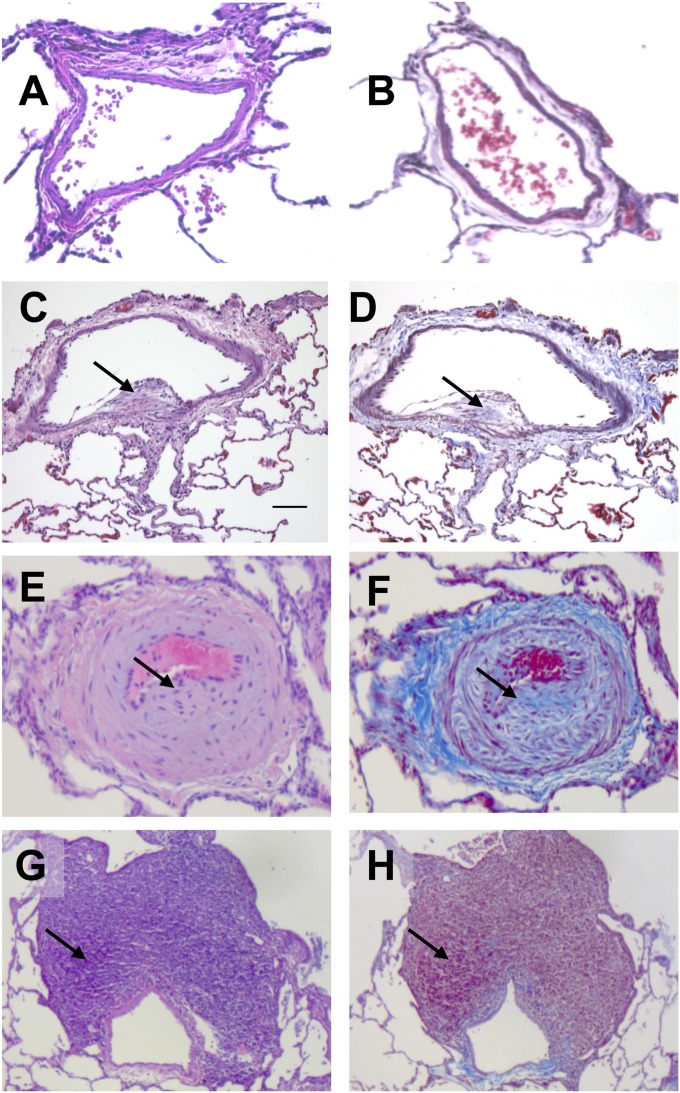
Pulmonary arterial hypertension (PAH) is increased in HIV, but its pathogenesis is not fully understood. Nonhuman primates infected with simian immunodeficiency virus (SIV) or SIV-HIV chimeric virus (SHIV) exhibit histologic changes characteristic of human PAH, but whether hemodynamic changes accompany this pathology is unknown. Repeated measurements of pulmonary artery pressures would permit longitudinal assessments of disease development and provide insights into pathogenesis. We tested the hypothesis that SIV-infected and SHIV-infected macaques develop physiologic manifestations of PAH. We performed right heart catheterizations, echocardiography, and computed tomography (CT) scans in macaques infected with either SIV (ΔB670) or SHIV (89.6P), and compared right heart and pulmonary artery pressures, as well as pulmonary vascular changes on CT scans, with those in uninfected control animals. Right atrial, right ventricular systolic, and pulmonary artery pressures (PAPs) were significantly elevated in 100% of macaques infected with either SIV or SHIV compared with control animals, with no difference in pulmonary capillary wedge pressure. PAPs increased as early as 3 months after SIV infection. Radiographic evidence of pulmonary vascular pruning was also found. Both SIV-infected and SHIV-infected macaques exhibited histologic changes in pulmonary arteries, predominantly consisting of intimal and medial hyperplasia. This report is the first to demonstrate SHIV-infected and SIV-infected macaques develop pulmonary hypertension at a high frequency, with physiologic changes occurring as early as 3 months after infection. These studies establish an important nonhuman primate model of HIV-associated PAH that will be useful in studies of disease pathogenesis and the efficacy of interventions.
Figures
Similar articles
-
Pulmonary vascular lesions are common in SIV- and SHIV-env-infected macaques.AIDS Res Hum Retroviruses. 2011 Feb;27(2):103-11. doi: 10.1089/aid.2009.0297. Epub 2010 Oct 21. AIDS Res Hum Retroviruses. 2011. PMID: 20961277 Free PMC article.
-
HIV-1 Nef is associated with complex pulmonary vascular lesions in SHIV-nef-infected macaques.Am J Respir Crit Care Med. 2006 Aug 15;174(4):437-45. doi: 10.1164/rccm.200601-005OC. Epub 2006 May 25. Am J Respir Crit Care Med. 2006. PMID: 16728715 Free PMC article.
-
Longitudinal Evaluation of Pulmonary Arterial Hypertension in a Rhesus Macaque (Macaca mulatta) Model of HIV Infection.Comp Med. 2018 Dec 1;68(6):461-473. doi: 10.30802/AALAS-CM-18-000012. Epub 2018 Dec 12. Comp Med. 2018. PMID: 30541636 Free PMC article.
-
[Use and research of pigtailed macaques in nonhuman primate HIV/AIDS models].Dongwuxue Yanjiu. 2013 Apr;34(2):77-88. doi: 10.3724/SP.J.1141.2013.02077. Dongwuxue Yanjiu. 2013. PMID: 23572356 Review. Chinese.
-
Nonhuman primate models for cell-associated simian immunodeficiency virus transmission: the need to better understand the complexity of HIV mucosal transmission.J Infect Dis. 2014 Dec 15;210 Suppl 3:S660-6. doi: 10.1093/infdis/jiu536. J Infect Dis. 2014. PMID: 25414421 Review.
Cited by
-
Vascular stiffness mechanoactivates YAP/TAZ-dependent glutaminolysis to drive pulmonary hypertension.J Clin Invest. 2016 Sep 1;126(9):3313-35. doi: 10.1172/JCI86387. Epub 2016 Aug 22. J Clin Invest. 2016. PMID: 27548520 Free PMC article.
-
The Latest in Animal Models of Pulmonary Hypertension and Right Ventricular Failure.Circ Res. 2022 Apr 29;130(9):1466-1486. doi: 10.1161/CIRCRESAHA.121.319971. Epub 2022 Apr 28. Circ Res. 2022. PMID: 35482834 Free PMC article. Review.
-
Maintaining lung health with longstanding HIV.Curr Opin Infect Dis. 2016 Feb;29(1):31-8. doi: 10.1097/QCO.0000000000000221. Curr Opin Infect Dis. 2016. PMID: 26555039 Free PMC article. Review.
-
Role of extracellular matrix in the pathogenesis of pulmonary arterial hypertension.Am J Physiol Heart Circ Physiol. 2018 Nov 1;315(5):H1322-H1331. doi: 10.1152/ajpheart.00136.2018. Epub 2018 Aug 24. Am J Physiol Heart Circ Physiol. 2018. PMID: 30141981 Free PMC article. Review.
-
CCR5 as a treatment target in pulmonary arterial hypertension.Circulation. 2014 Sep 9;130(11):880-891. doi: 10.1161/CIRCULATIONAHA.114.010757. Epub 2014 Jul 3. Circulation. 2014. PMID: 24993099 Free PMC article.
References
-
- Speich R, Jenni R, Opravil M, Pfab M, Russi EW. Primary pulmonary hypertension in HIV infection. Chest 1991;100:1268–1271 - PubMed
-
- Sitbon O, Lascoux-Combe C, Delfraissy JF, Yeni PG, Raffi F, De Zuttere D, Gressin V, Clerson P, Sereni D, Simonneau G. Prevalence of HIV-related pulmonary arterial hypertension in the current antiretroviral therapy era. Am J Respir Crit Care Med 2008;177:108–113 - PubMed
-
- Cicalini S, Almodovar S, Grilli E, Flores S. Pulmonary hypertension and human immunodeficiency virus infection: epidemiology, pathogenesis, and clinical approach. Clin Microbiol Infect 2011;17:25–33 - PubMed
-
- Mondy KE, Gottdiener J, Overton ET, Henry K, Bush T, Conley L, Hammer J, Carpenter CC, Kojic E, Patel P, et al. High prevalence of echocardiographic abnormalities among HIV-infected persons in the era of highly active antiretroviral therapy. Clin Infect Dis 2011;52:378–386 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
