

Exhaled air dispersion during coughing with and without wearing a surgical or N95 mask
- PMID: 23239991
- PMCID: PMC3516468
- DOI: 10.1371/journal.pone.0050845
Exhaled air dispersion during coughing with and without wearing a surgical or N95 mask
Abstract
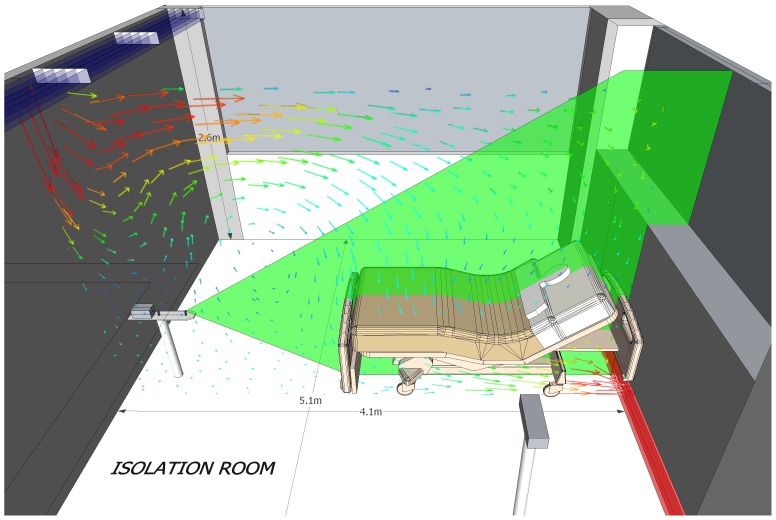
Objectives: We compared the expelled air dispersion distances during coughing from a human patient simulator (HPS) lying at 45° with and without wearing a surgical mask or N95 mask in a negative pressure isolation room.
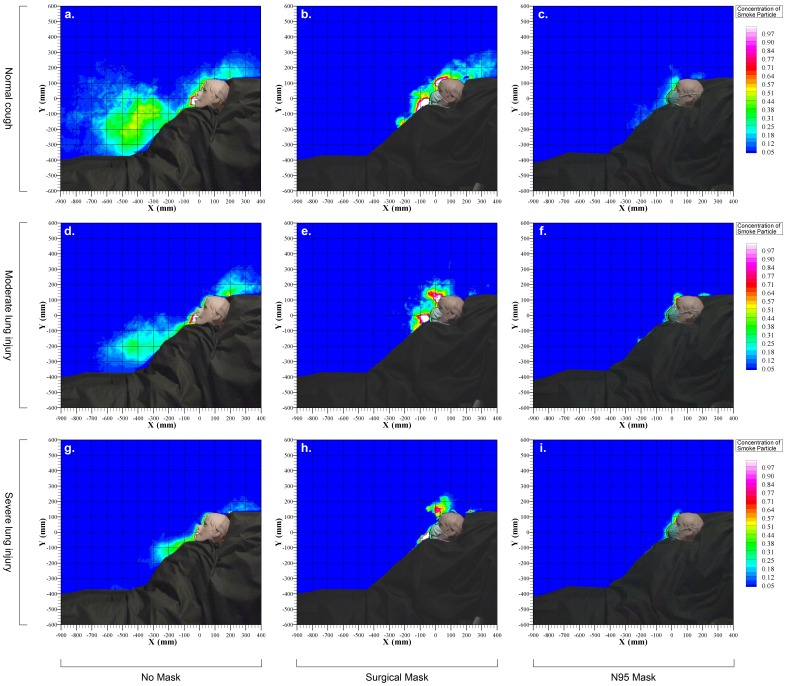
Methods: Airflow was marked with intrapulmonary smoke. Coughing bouts were generated by short bursts of oxygen flow at 650, 320, and 220L/min to simulate normal, mild and poor coughing efforts, respectively. The coughing jet was revealed by laser light-sheet and images were captured by high definition video. Smoke concentration in the plume was estimated from the light scattered by smoke particles. Significant exposure was arbitrarily defined where there was ≥ 20% of normalized smoke concentration.
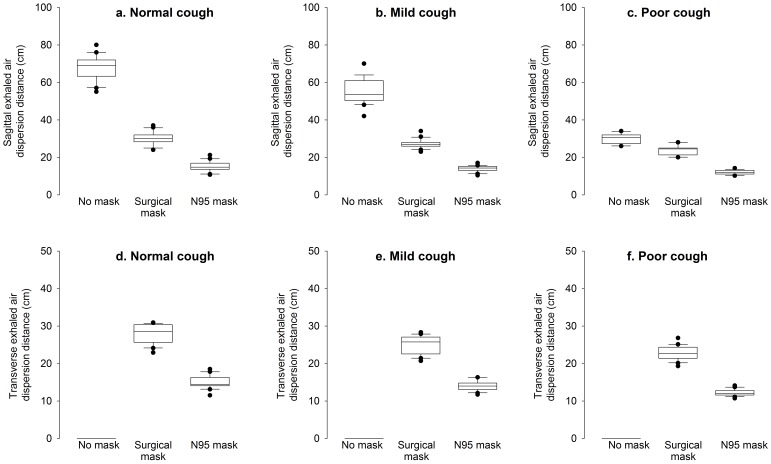
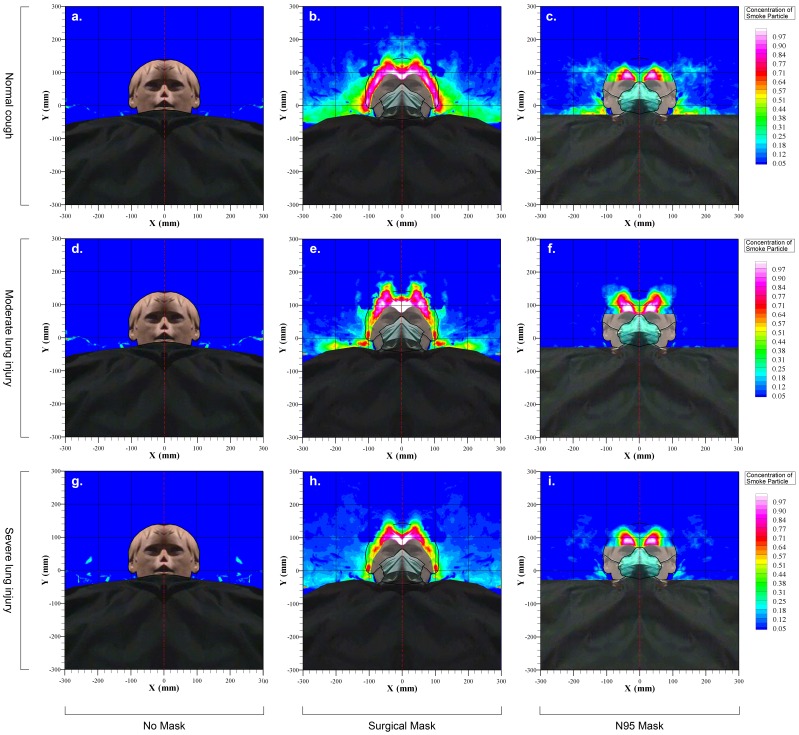
Results: During normal cough, expelled air dispersion distances were 68, 30 and 15 cm along the median sagittal plane when the HPS wore no mask, a surgical mask and a N95 mask, respectively. In moderate lung injury, the corresponding air dispersion distances for mild coughing efforts were reduced to 55, 27 and 14 cm, respectively, p < 0.001. The distances were reduced to 30, 24 and 12 cm, respectively during poor coughing effort as in severe lung injury. Lateral dispersion distances during normal cough were 0, 28 and 15 cm when the HPS wore no mask, a surgical mask and a N95 mask, respectively.
Conclusions: Normal cough produced a turbulent jet about 0.7 m towards the end of the bed from the recumbent subject. N95 mask was more effective than surgical mask in preventing expelled air leakage during coughing but there was still significant sideway leakage.
Conflict of interest statement
Figures
References
-
- Musher DM (2003) How contagious are common respiratory tract infections? N Engl J Med 348: 1256–1266. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
