

Penile revascularization--contemporary update
- PMID: 23241636
- PMCID: PMC3739123
- DOI: 10.1038/aja.2012.146
Penile revascularization--contemporary update
Abstract
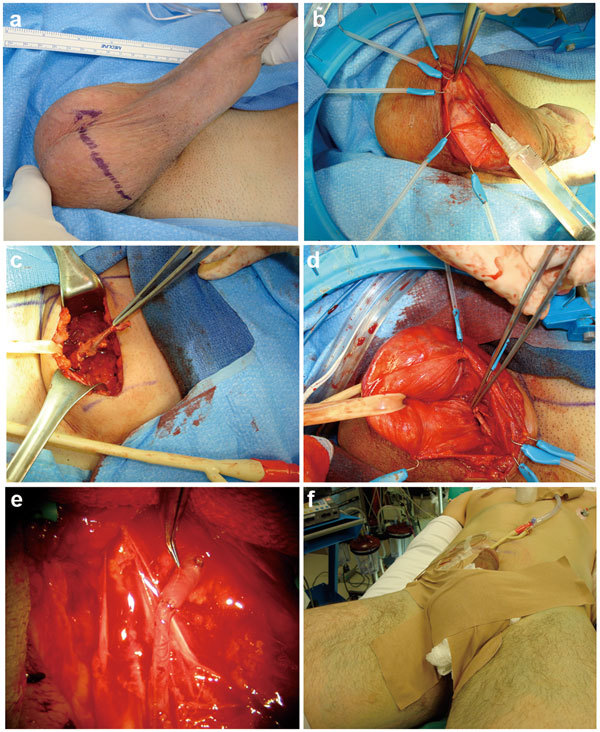
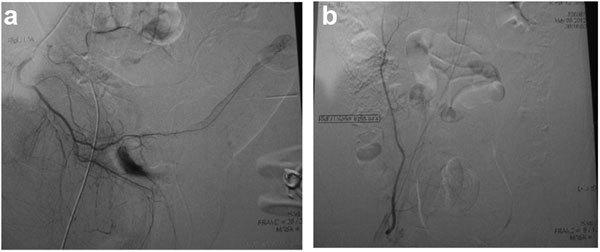
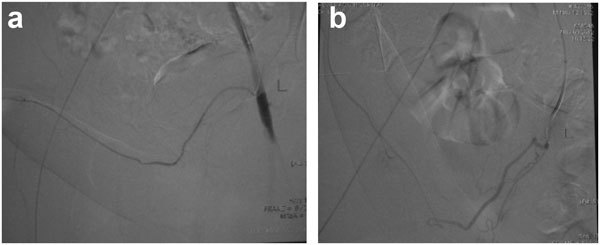
Contemporary therapies for erectile dysfunction are generally targeted towards older men and universally engage pharmacological and/or device related treatment options. Penile revascularization, using microvascular arterial bypass surgical techniques, is a non-pharmacological, non-device-related, and reconstructive surgical strategy for men with erectile dysfunction that was first described by Dr Vaclav Michal in 1973. Contemporary penile revascularization attempts to 'cure' pure arteriogenic erectile dysfunction in young men with arterial occlusive pathology in the distal internal pudendal, common penile or proximal cavernosal artery secondary to focal endothelial injury from blunt pelvic, perineal or penile trauma. A microvascular anastomosis is fashioned between the donor inferior epigastric and recipient dorsal penile artery. Increased perfusion pressure is theoretically communicated to the cavernosal artery via perforating branches from the dorsal artery. This article will review the history, indications and pathophysiology of blunt trauma-induced focal arterial occlusive disease in young men with erectile dysfunction, current surgical techniques utilized and results of surgery. Contemporary use of penile revascularization is a logical and wanted therapeutic option to attempt to reverse erectile dysfunction in young men who have sustained blunt pelvic, perineal or penile trauma.
Figures
References
-
- Michal V, Kramár R, Pospíchal J, Hejhal L.[Direct arterial anastomosis on corpora cavernosa penis in the therapy of erective impotence.] Rozhl Chir 197352587–90.Czech. - PubMed
-
- Michal V, Kramár R, Pospíchal J. Femoro-pudendal by-pass, internal iliac thromboendarterectomy and direct arterial anastomosis to the cavernous body in the treatment of erectile impotence. Bull Soc Int Chir. 1974;33:343–50. - PubMed
-
- Michal V. Arterial disease as a cause of impotence. Clin Endocrinol Metab. 1982;11:725–48. - PubMed
-
- Kayıgil O, Okulu E, Aldemir M, Onen E. Penile revascularization in vasculogenic erectile dysfunction (ED): long-term follow-up. BJU Int. 2011;109:109–15. - PubMed
-
- Sarramon JP, Malavaud B, Braud F, Bertrand N, Vaessen C, et al. Evaluation of male sexual function by the International Index of Erectile Function after deep dorsal vein arterialization of the penis. J Urol. 2001;166:576–80. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
