

A randomized study of remote follow-up of implantable cardioverter defibrillators: safety and efficacy report of the ECOST trial
- PMID: 23242192
- PMCID: PMC3578267
- DOI: 10.1093/eurheartj/ehs425
A randomized study of remote follow-up of implantable cardioverter defibrillators: safety and efficacy report of the ECOST trial
Abstract
Aims: The ECOST trial examined prospectively the long-term safety and effectiveness of home monitoring (HM) of implantable cardioverter defibrillators (ICD).
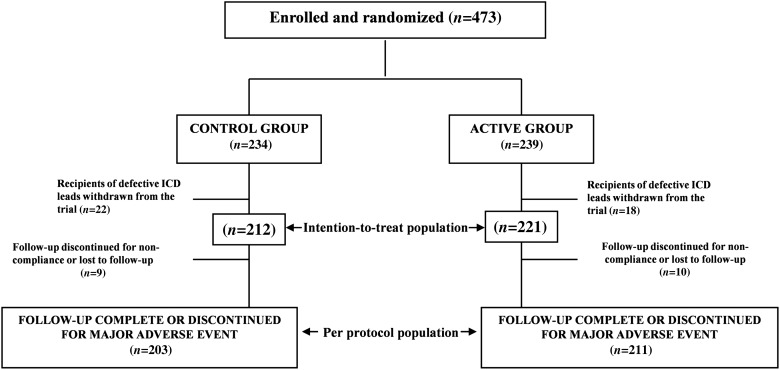
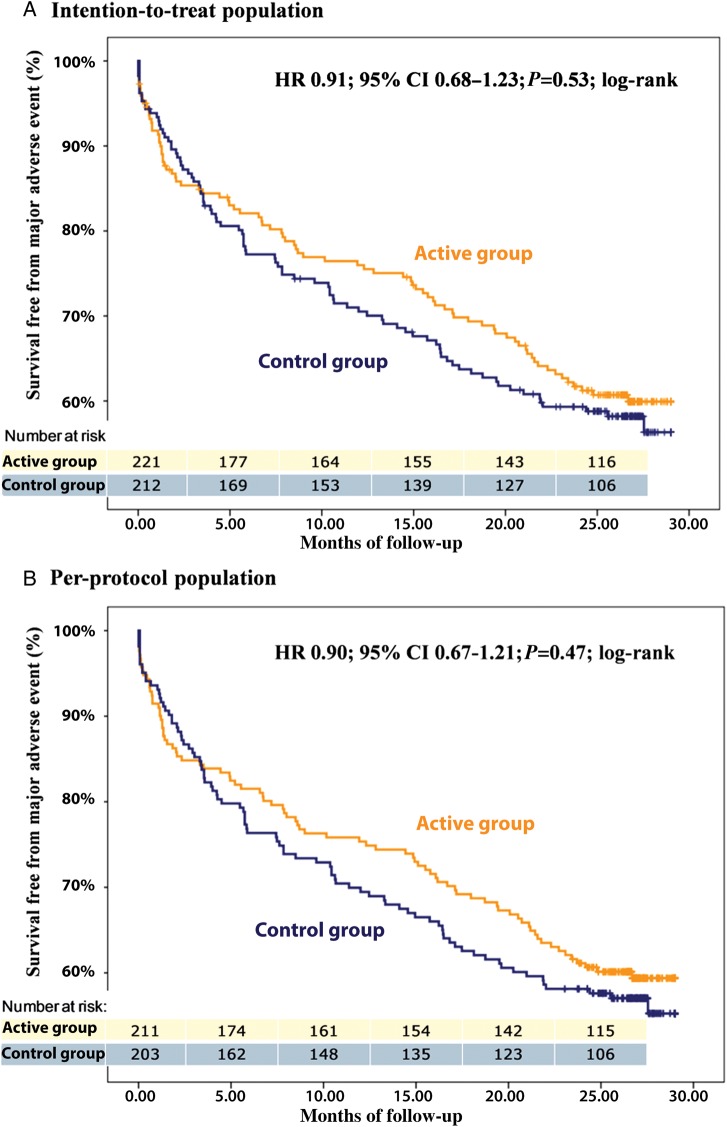
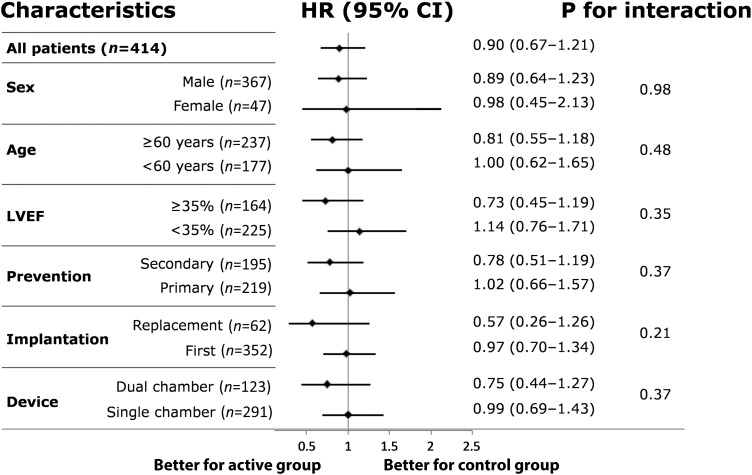
Methods and results: The trial's primary objective was to randomly compare the proportions of patients experiencing ≥ 1 major adverse event (MAE), including deaths from all causes, and cardiovascular, procedure-related, and device-related MAE associated with HM (active group) vs. ambulatory follow-ups (control group) in a sample of 433 patients. The 221 patients assigned to the active group were seen once a year, unless HM reported an ICD dysfunction or a clinical event requiring an ambulatory visit, while the 212 patients in the control group underwent ambulatory visits every 6 months. The characteristics of the study groups were similar. Over a follow-up of 24.2 months, 38.5% of patients in the active and 41.5% in the control group experienced ≥ 1 MAE (P < 0.05 for non-inferiority). The overall number of shocks delivered was significantly lower in the active (n = 193) than in the control (n = 657) group (P < 0.05) and the proportion of patients who received inappropriate shocks was 52% lower in the active (n = 11) than in the control (n = 22) group (P < 0.05). At the end of the follow-up, the battery longevity was longer in the active group because of a lower number of capacitor charges (499 vs. 2081).
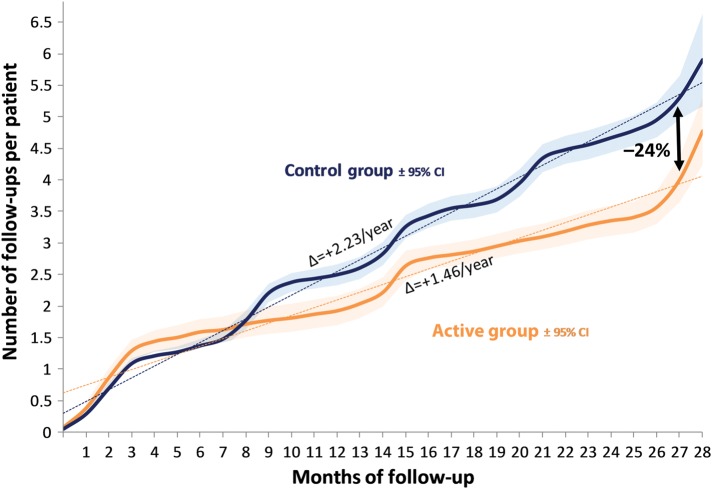
Conclusion: Our observations indicate that long-term HM of ICD is at least as safe as standard ambulatory follow-ups with respect to a broad spectrum of MAE. It also lowered significantly the number of appropriate and inappropriate shocks delivered, and spared the device battery. Clinical trials registration NCT00989417.
Figures
Comment in
-
Remote monitoring of patients with Implantable Cardioverter Defibrillators (ICD): a cute gimmick or an essential tool for clinical excellence?J Cardiovasc Electrophysiol. 2014 Jul;25(7):771-3. doi: 10.1111/jce.12415. Epub 2014 May 2. J Cardiovasc Electrophysiol. 2014. PMID: 24654708 No abstract available.
References
-
- ICT for better healthcare in Europe. http://ec.europa.eu/information_society/activities/health/index_en.htm. 18 June 2012.
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA, III, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Faxon DP, Halperin JL, Hiratzka LF, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura RA, Ornato JP, Page RL, Riegel B, Tarkington LG, Yancy CW American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices); American Association for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008;117:2820–2840. doi:10.1161/CIRCUALTIONAHA.108.189741. - DOI - PubMed
-
- Brugada P. What evidence do we have to replace in-hospital implantable cardioverter defibrillator follow-up? Clin Res Cardiol. 2006;95(Suppl. 3):III/3–9. - PubMed
-
- Heidbüchel H, Lioen P, Foulon S, Huybrechts W, Ector J, Willems R, Ector H. Potential role of remote monitoring for scheduled and unscheduled evaluations of patients with an implantable defibrillator. Europace. 2008;10:351–357. doi:10.1093/europace/eun010. - DOI - PubMed
-
- Nielsen JC, Kottkamp H, Zabel M, Aliot E, Kreutzer U, Bauer A, Schuchert A, Neuser H, Schumacher B, Schmidinger H, Stix G, Clémenty J, Danilovic D, Hindricks G. Automatic home monitoring of implantable cardioverter defibrillators. Europace. 2008;10:729–735. doi:10.1093/europace/eun099. - DOI - PubMed
