

Real-time multi-modality imaging of glioblastoma tumor resection and recurrence
- PMID: 23242736
- PMCID: PMC3548430
- DOI: 10.1007/s11060-012-1008-z
Real-time multi-modality imaging of glioblastoma tumor resection and recurrence
Abstract
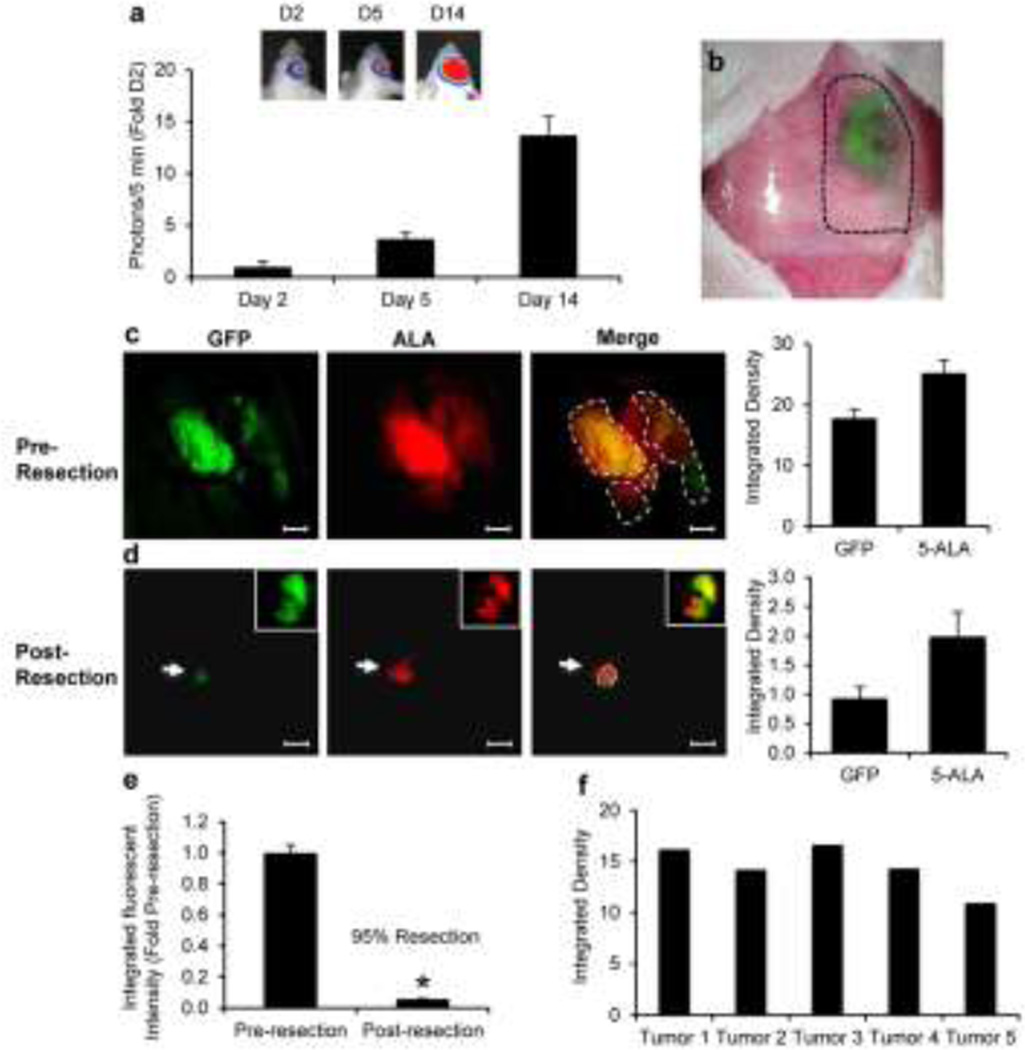
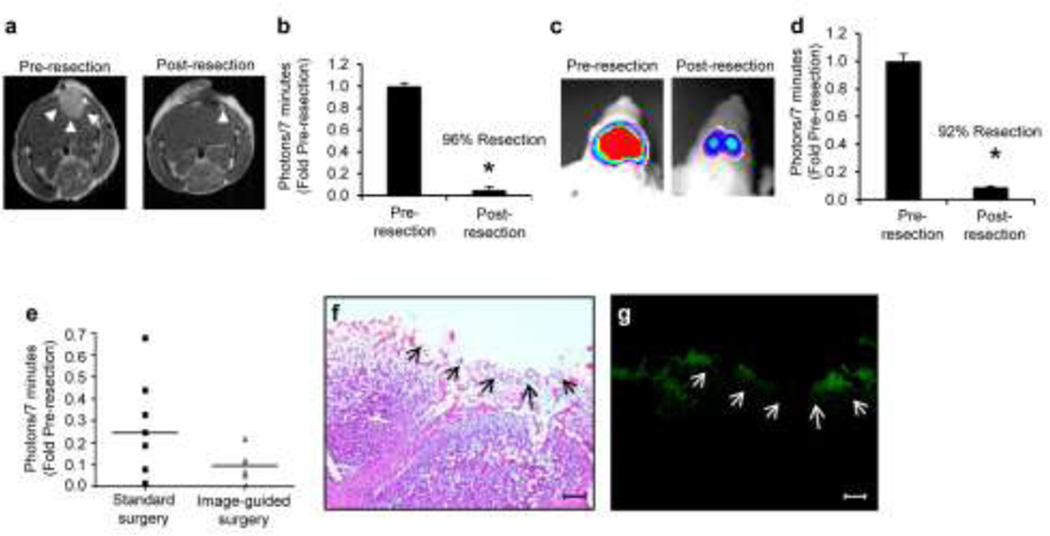
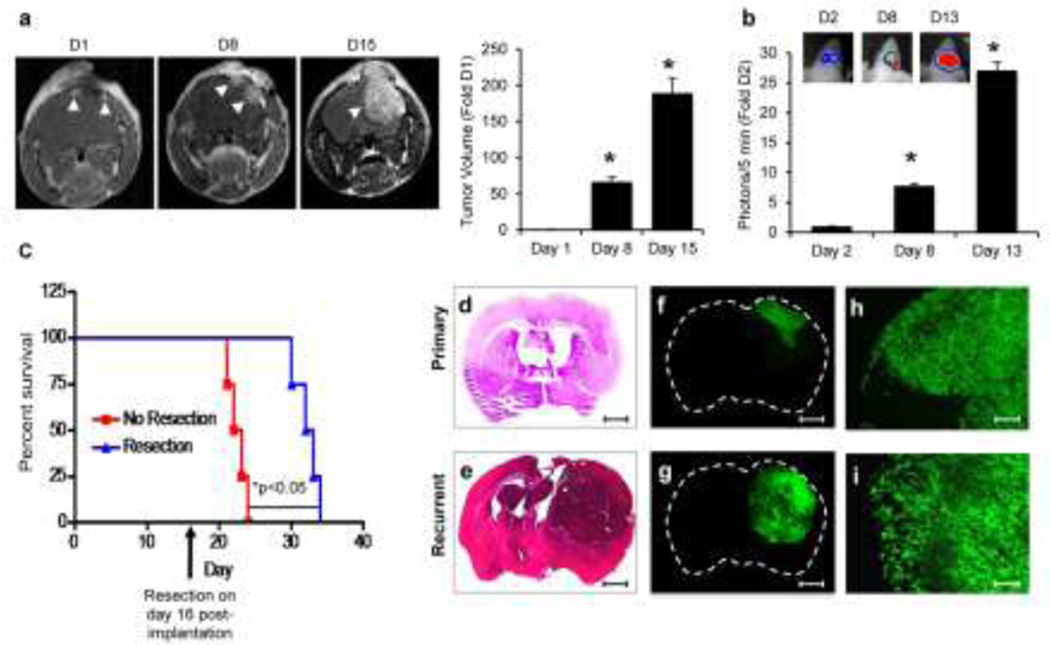
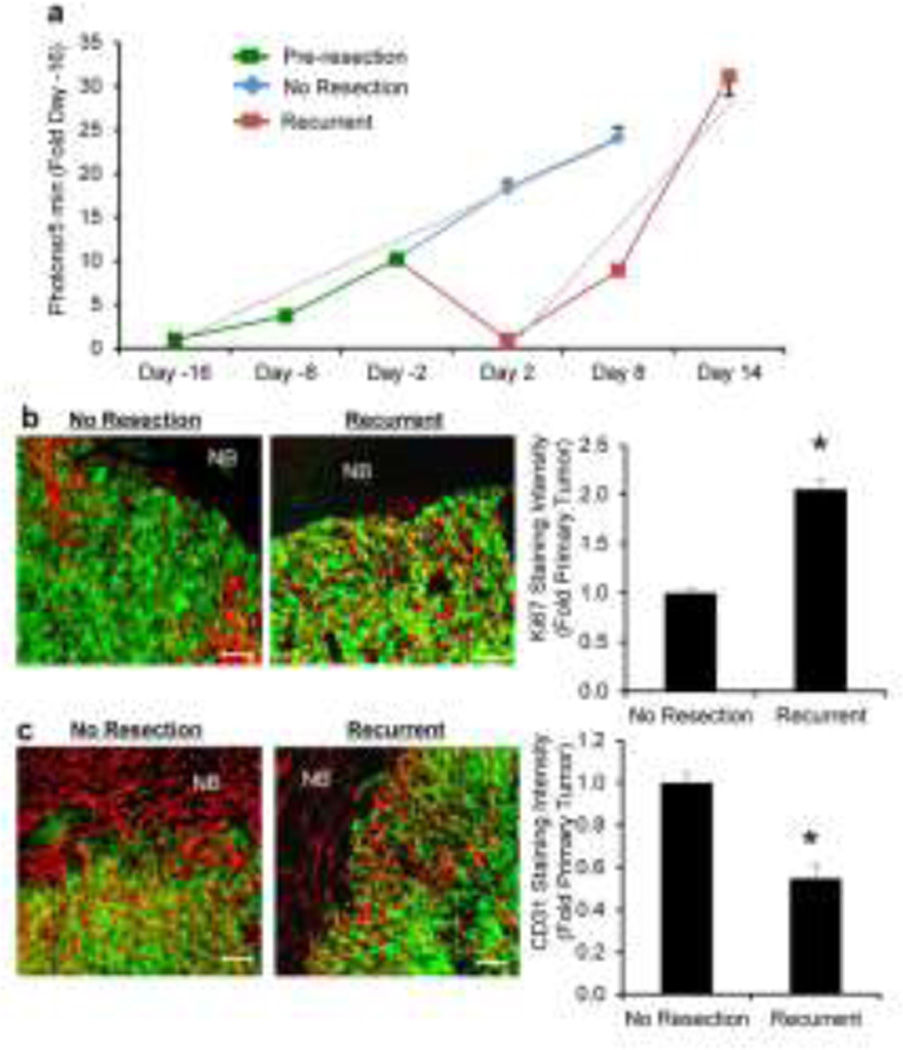
The lack of relevant pre-clinical animal models incorporating the clinical scenario of Glioblastoma multiforme (GBM) resection and recurrence has contributed significantly to the inability to successfully treat GBM. A multi-modality imaging approach that allows real-time assessment of tumor resection during surgery and non-invasive detection of post-operative tumor volumes is urgently needed. In this study, we report the development and implementation of an optical imaging and magnetic resonance imaging (MRI) approach to guide GBM resection during surgery and track tumor recurrence at multiple resolutions in mice. Intra-operative fluorescence-guided surgery allowed real-time monitoring of intracranial tumor removal and led to greater than 90 % removal of established intracranial human GBM. The fluorescent signal clearly delineated tumor margins, residual tumor, and correlated closely with the clinically utilized fluorescence surgical marker 5-aminolevulinic acid/porphyrin. Post-operative non-invasive optical imaging and MRI confirmed near-complete tumor removal, which was further validated by immunohistochemistry (IHC). Longitudinal non-invasive imaging and IHC showed rapid recurrence of multi-focal tumors that exhibited a faster growth rate and altered blood-vessel density compared to non-resected tumors. Surgical tumor resection significantly extended long-term survival, however mice ultimately succumbed to the recurrent GBM. This multi-modality imaging approach to GBM resection and recurrence in mice should provide an important platform for investigating multiple aspects of GBM and ultimately evaluating novel therapeutics.
Conflict of interest statement
Figures
References
-
- Adamson C, Kanu OO, Mehta AI, Di C, Lin N, Mattox AK, Bigner DD. Glioblastoma multiforme: a review of where we have been and where we are going. Expert Opin Investig Drugs. 2009;18:1061–1083. - PubMed
-
- Asthagiri AR, Pouratian N, Sherman J, Ahmed G, Shaffrey ME. Advances in brain tumor surgery. Neurol Clin. 2007;25:975–1003. viii-ix, - PubMed
-
- Lacroix M, Abi-Said D, Fourney DR, Gokaslan ZL, Shi W, DeMonte F, Lang FF, McCutcheon IE, Hassenbusch SJ, Holland E, Hess K, Michael C, Miller D, Sawaya R. A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. Journal of neurosurgery. 2001;95:190–198. - PubMed
-
- Stark AM, Nabavi A, Mehdorn HM, Blomer U. Glioblastoma multiforme-report of 267 cases treated at a single institution. Surg Neurol. 2005;63:162–169. discussion 169. - PubMed
-
- Fomchenko EI, Holland EC. Mouse models of brain tumors and their applications in preclinical trials. Clin Cancer Res. 2006;12:5288–5297. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
