

Prognostic impact of (18)FDG-PET-CT findings in clinical stage III and IIB breast cancer
- PMID: 23243198
- PMCID: PMC3525816
- DOI: 10.1093/jnci/djs451
Prognostic impact of (18)FDG-PET-CT findings in clinical stage III and IIB breast cancer
Abstract
Background: This study prospectively evaluated the yield of fluorodeoxyglucose positron emission tomography/computed tomography ((18)FDG-PET-CT) in patients with clinical stages II and III breast cancer and the impact of PET-CT results on prognosis.
Methods: In the course of 71 months, 254 consecutive patients with clinical stages II and III breast cancer (based on clinical examination, mammography, breast magnetic resonance imaging, and locoregional ultrasonography) underwent (18)FDG-PET-CT. The yield was assessed in the whole population and for each American Joint Committee on Cancer subgroup. The prognostic impact of PET-CT findings was analyzed. Tests of statistical significance were two-sided.
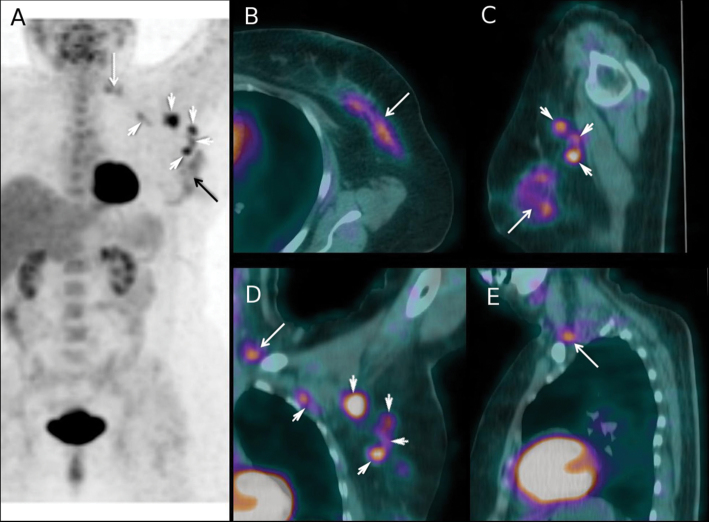
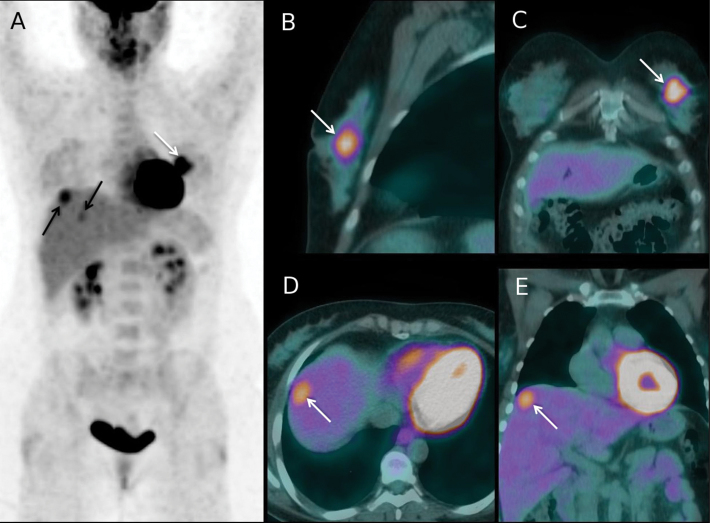
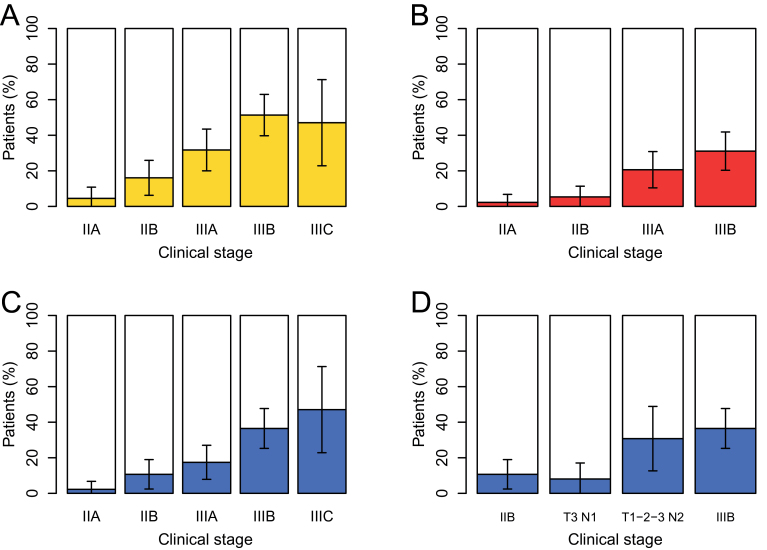
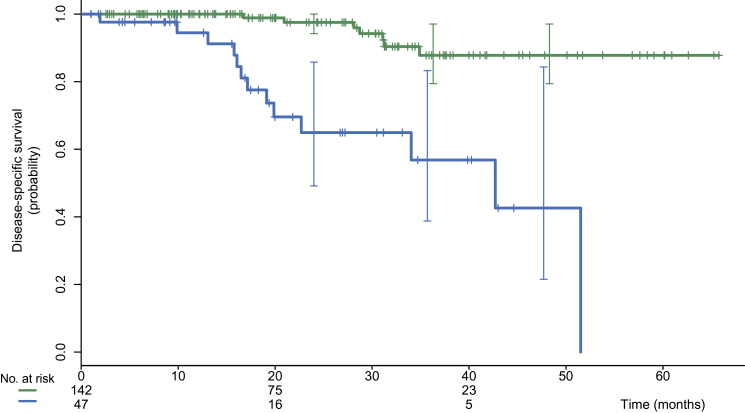
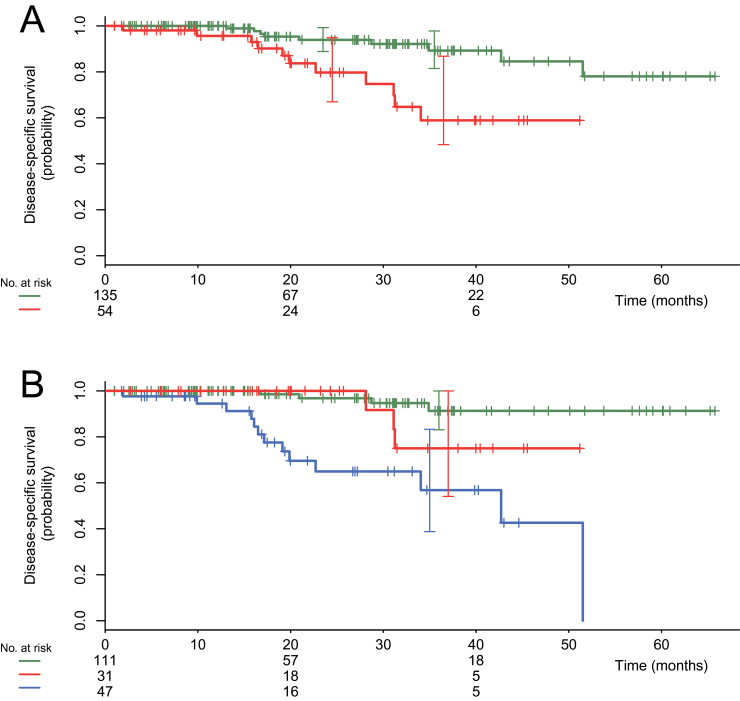
Results: (18)FDG-PET-CT changed the clinical stage in 77 of 254 patients (30.3%; 95% confidence interval [CI] = 25.0% to 36.2%). It showed unsuspected N3 disease (infraclavicular, supraclavicular, or internal mammary nodes) in 40 patients and distant metastases in 53. PET-CT revealed distant metastases in 2.3% (1 of 44) of clinical stage IIA, 10.7% (6 of 56) of stage IIB, 17.5% (11 of 63) of stage IIIA, 36.5% (27 of 74) of stage IIIB, and 47.1% (8 of 17) of stage IIIC patients. Among 189 patients with clinical stage IIB or higher disease and adequate follow-up, disease-specific survival was statistically significantly shorter in the 47 patients scored M1 on (18)FDG-PET-CT in comparison with those scored M0, with a three-year disease-specific survival of 57% vs 88% (P < .001). In multivariable analysis, only distant disease on PET-CT and triple-negative phenotype were statistically significant prognostic factors. The relative risk of death was 26.60 (95% CI = 6.60 to 102.62) for M1 vs M0 patients.
Conclusions: The yield of (18)FDG-PET-CT appeared substantial in patients with clinical stage IIB or higher breast cancer. In these patients, (18)FDG-PET-CT provided powerful prognostic stratification.
Figures
Comment in
-
Evaluating the impact of new imaging tests: promises and pitfalls.J Natl Cancer Inst. 2012 Dec 19;104(24):1857-8. doi: 10.1093/jnci/djs488. Epub 2012 Dec 12. J Natl Cancer Inst. 2012. PMID: 23243197 No abstract available.
References
-
- Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual. 7thed. New York: Springer; 2010;.
-
- Groheux D, Hindié E, Rubello D, et al. Should FDG PET/CT be used for the initial staging of breast cancer?. Eur J Nucl Med Mol Imaging. 2009; 36(10):1539–1542 - PubMed
-
- Hindié E, Groheux D, Brenot-Rossi I, Rubello D, Moretti JL, Espié M. The sentinel node procedure in breast cancer: nuclear medicine as the starting point. J Nucl Med. 2011; 52(3):405–414 - PubMed
-
- Yang WT, Le-Petross HT, Macapinlac H, et al. Inflammatory breast cancer: PET/CT, MRI, mammography, and sonography findings. Breast Cancer Res Treat. 2008; 109(3):417–426 - PubMed
-
- Carkaci S, Macapinlac HA, Cristofanilli M, et al. Retrospective study of 18F-FDG PET/CT in the diagnosis of inflammatory breast cancer: preliminary data. J Nucl Med. 2009; 50(2):231–238 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
