

DNA methylation as an adjunct to histopathology to detect prevalent, inconspicuous dysplasia and early-stage neoplasia in Barrett's esophagus
- PMID: 23243219
- PMCID: PMC4998953
- DOI: 10.1158/1078-0432.CCR-12-2880
DNA methylation as an adjunct to histopathology to detect prevalent, inconspicuous dysplasia and early-stage neoplasia in Barrett's esophagus
Abstract
Purpose: Endoscopic surveillance of Barrett's esophagus is problematic because dysplasia/early-stage neoplasia is frequently invisible and likely to be missed because of sampling bias. Molecular abnormalities may be more diffuse than dysplasia. The aim was therefore to test whether DNA methylation, especially on imprinted and X-chromosome genes, is able to detect dysplasia/early-stage neoplasia.
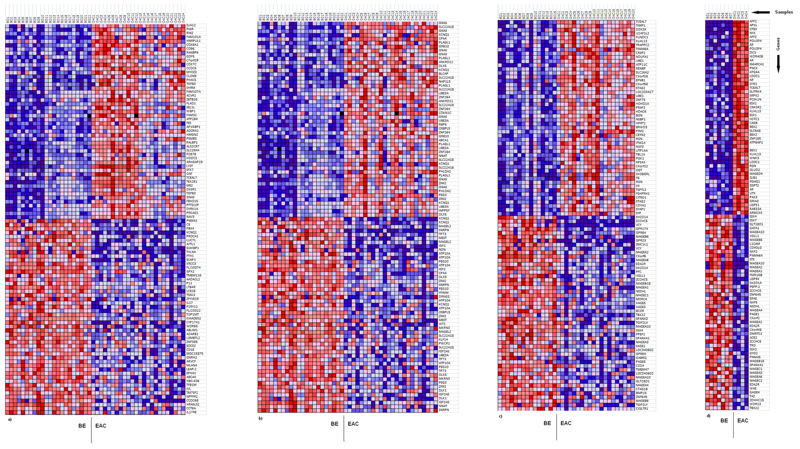
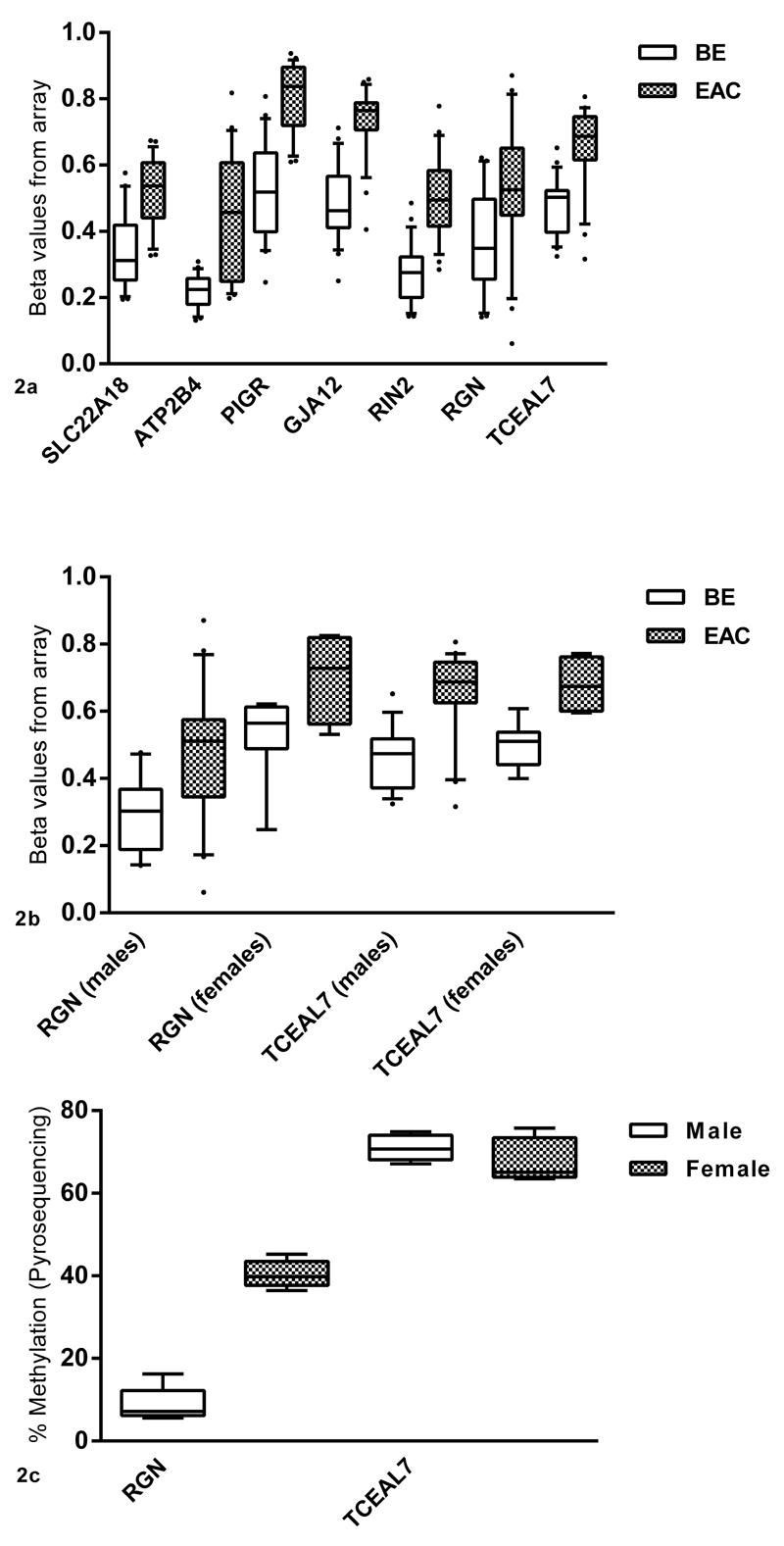
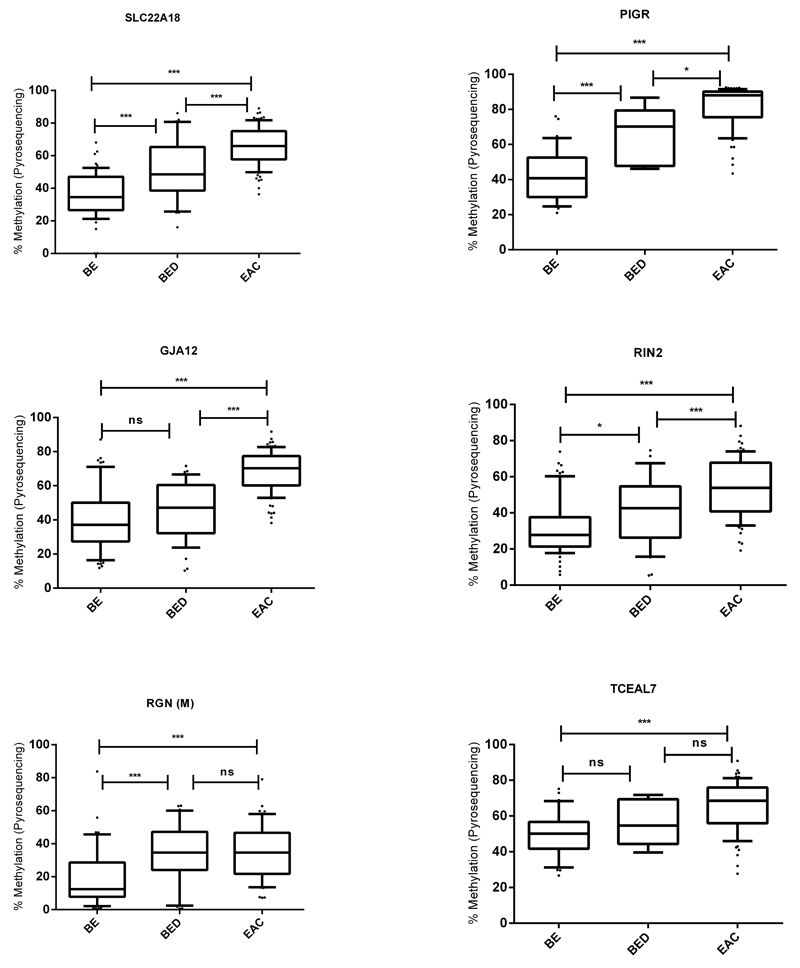
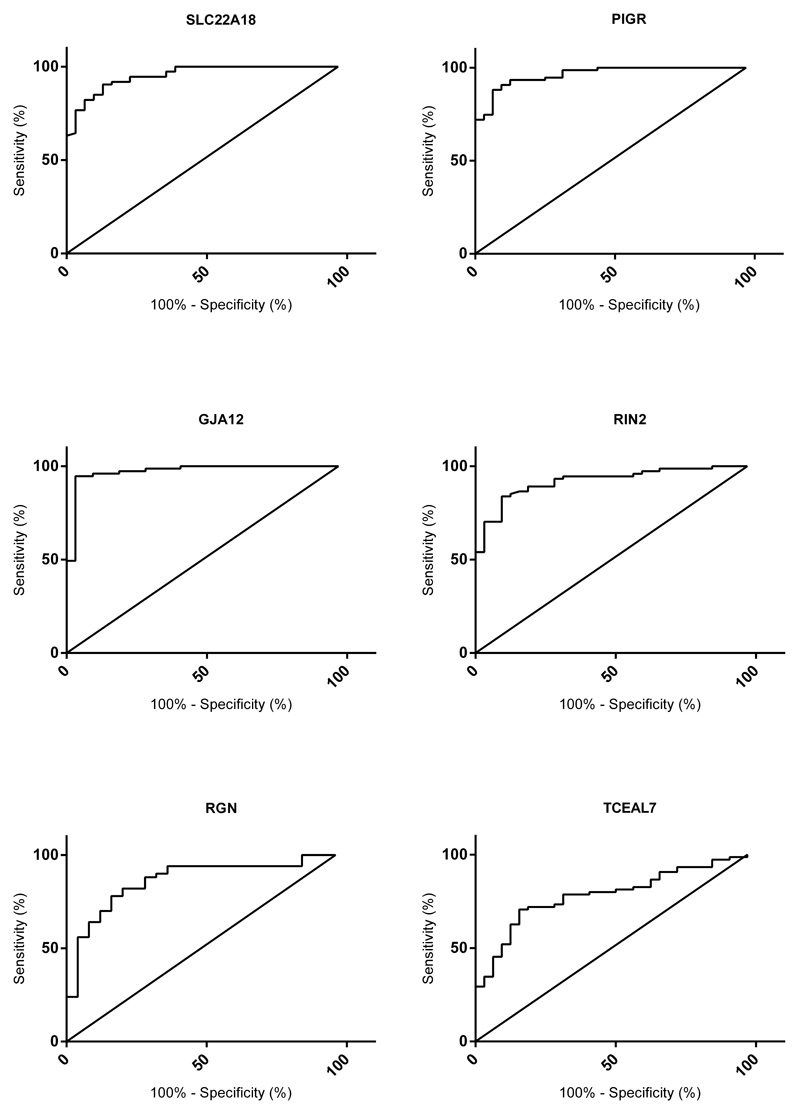
Experimental design: 27K methylation arrays were used to find genes best able to differentiate between 22 Barrett's esophagus and 24 esophageal adenocarcinoma (EAC) samples. These were validated using pyrosequencing on a retrospective cohort (60 Barrett's esophagus, 36 dysplastic, and 90 EAC) and then in a prospective multicenter study (98 Barrett's esophagus patients, including 28 dysplastic and 9 early EAC) designed to utilize biomarkers to stratify patients according to their prevalent dysplasia/EAC status.
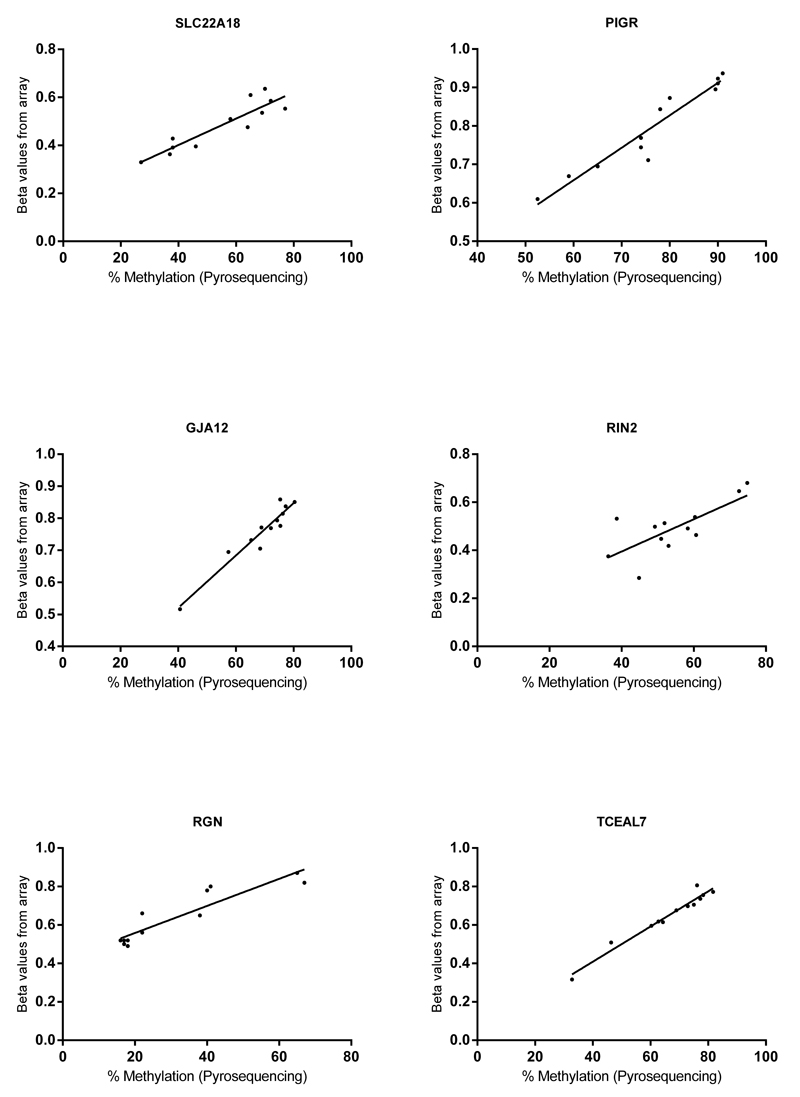
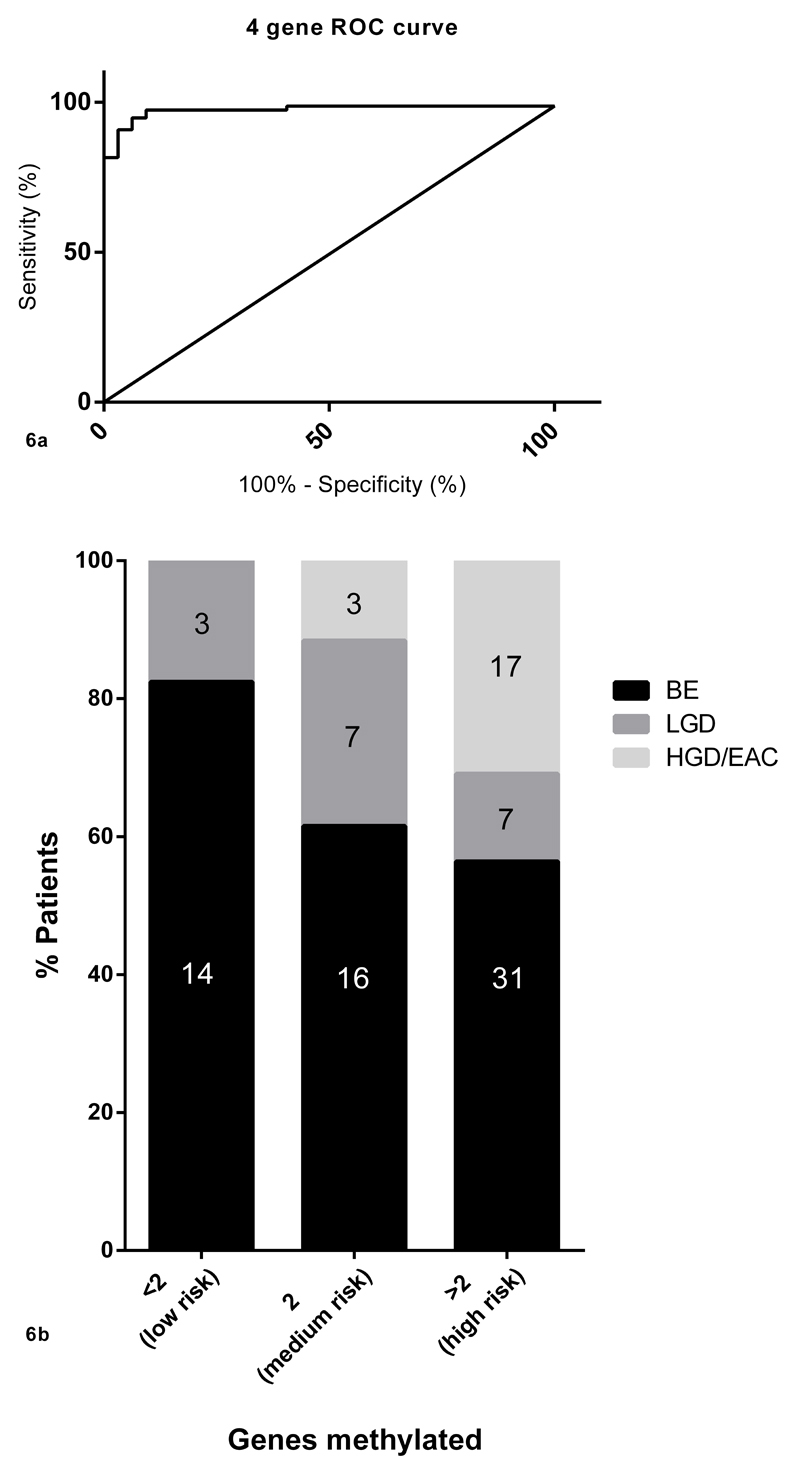
Results: Genes (23%) on the array, including 7% of X-linked and 69% of imprinted genes, have shown statistically significant changes in methylation in EAC versus Barrett's esophagus (Wilcoxon P < 0.05). 6/7 selected candidate genes were successfully internally (Pearson's P < 0.01) and externally validated (ANOVA P < 0.001). Four genes (SLC22A18, PIGR, GJA12, and RIN2) showed the greatest area under curve (0.988) to distinguish between Barrett's esophagus and dysplasia/EAC in the retrospective cohort. This methylation panel was able to stratify patients from the prospective cohort into three risk groups based on the number of genes methylated (low risk: <2 genes, intermediate: 2, and high: >2).
Conclusion: Widespread DNA methylation changes were observed in Barrett's carcinogenesis including ≈70% of known imprinted genes. A four-gene methylation panel stratified patients with Barrett's esophagus into three risk groups with potential clinical utility.
©2012 AACR.
Conflict of interest statement
There is no conflict of interest to declare.
Figures
References
-
- Hvid-Jensen F, Pedersen L, Drewes AM, Sørensen HT, Funch-Jensen P. Incidence of Adenocarcinoma among Patients with Barrett's Esophagus. New England Journal of Medicine. 2011;365:1375–83. - PubMed
-
- Pohl H, Sirovich B, Welch HG. Esophageal Adenocarcinoma Incidence: Are We Reaching the Peak? Cancer Epidemiology Biomarkers & Prevention. 2010;19:1468–70. - PubMed
-
- DeMeester S. Evaluation and Treatment of Superficial Esophageal Cancer. Journal of Gastrointestinal Surgery. 2010;14:94–100. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
