

Treatment and outcomes of an Australian cohort of outpatients with bipolar I or schizoaffective disorder over twenty-four months: implications for clinical practice
- PMID: 23244301
- PMCID: PMC3570370
- DOI: 10.1186/1471-244X-12-228
Treatment and outcomes of an Australian cohort of outpatients with bipolar I or schizoaffective disorder over twenty-four months: implications for clinical practice
Abstract
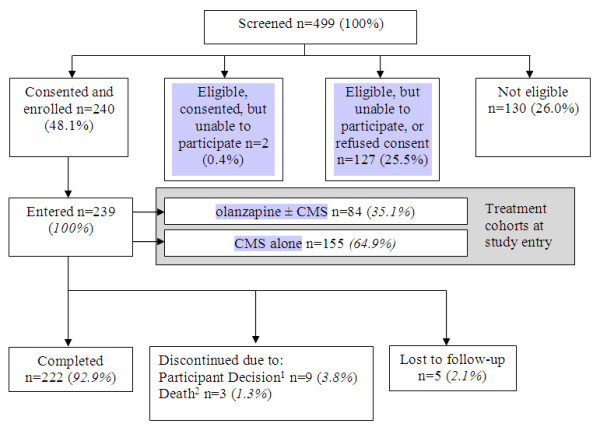
Background: The Bipolar Comprehensive Outcomes Study (BCOS) is a 2-year, prospective, non-interventional, observational study designed to explore the clinical and functional outcomes associated with 'real-world' treatment of participants with bipolar I or schizoaffective disorder. All participants received treatment as usual. There was no study medication.
Methods: Participants prescribed either conventional mood stabilizers (CMS; n = 155) alone, or olanzapine with, or without, CMS (olanzapine ± CMS; n = 84) were assessed every 3 months using several measures, including the Young Mania Rating Scale, 21-item Hamilton Depression Rating Scale, Clinical Global Impressions Scale - Bipolar Version, and the EuroQol Instrument. This paper reports 24-month longitudinal clinical, pharmacological, functional, and socioeconomic data.
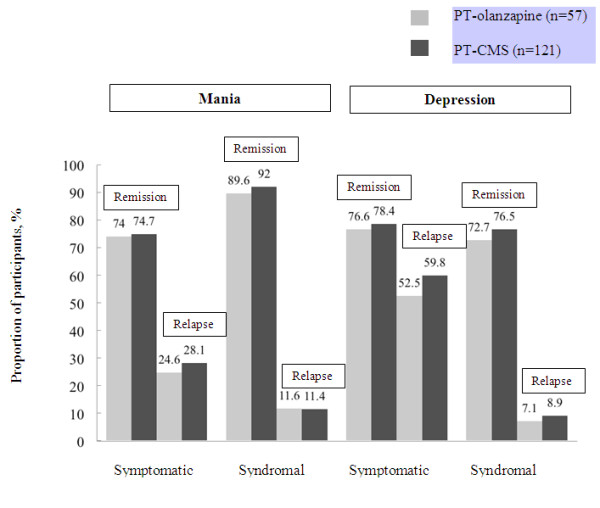
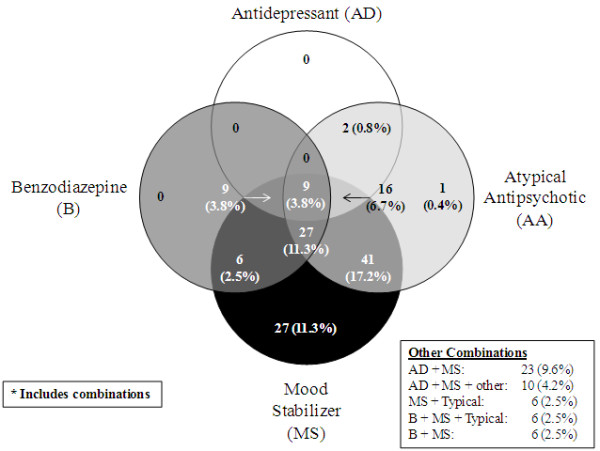
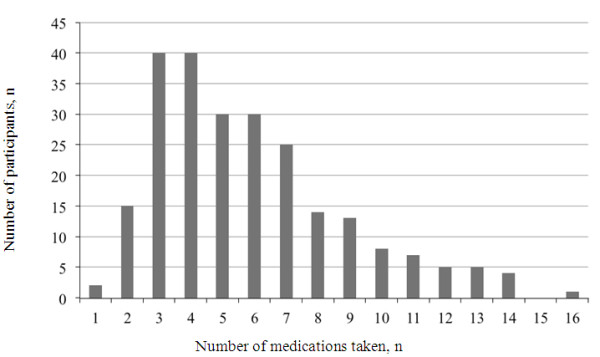
Results: On average, participants were 42 (range 18 to 79) years of age, 58%; were female, and 73%; had a diagnosis of bipolar I. Polypharmacy was the usual approach to pharmacological treatment; participants took a median of 5 different psychotropic medications over the course of the study, and spent a median proportion of time of 100%; of the study on mood stabilizers, 90%; on antipsychotics, 9%; on antidepressants, and 5%; on benzodiazepines/hypnotics. By 24 months, the majority of participants had achieved both symptomatic and syndromal remission of both mania and depression. Symptomatic relapse rates were similar for both the CMS alone (65%;) and the olanzapine ± CMS (61%;) cohorts.
Conclusions: Participants with bipolar I or schizoaffective disorder in this study were receiving complex medication treatments that were often discordant with recommendations made in contemporary major treatment guidelines. The majority of study participants demonstrated some clinical and functional improvements, but not all achieved remission of symptoms or syndrome.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
