

Update on the theory and management of orthostatic intolerance and related syndromes in adolescents and children
- PMID: 23244360
- PMCID: PMC3896077
- DOI: 10.1586/erc.12.139
Update on the theory and management of orthostatic intolerance and related syndromes in adolescents and children
Abstract
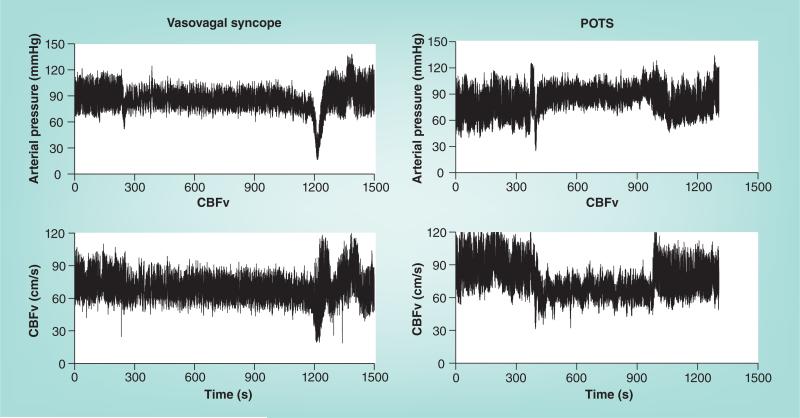
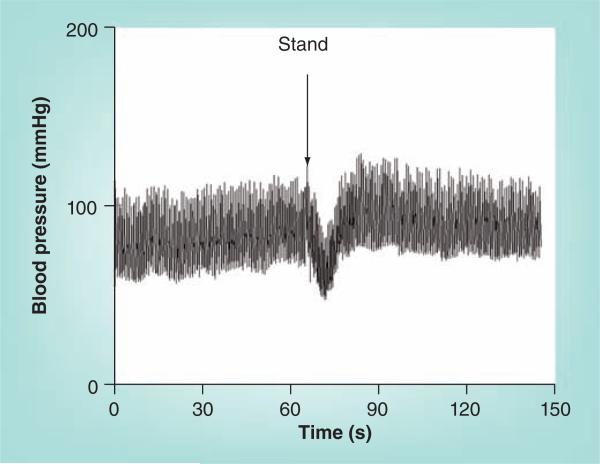
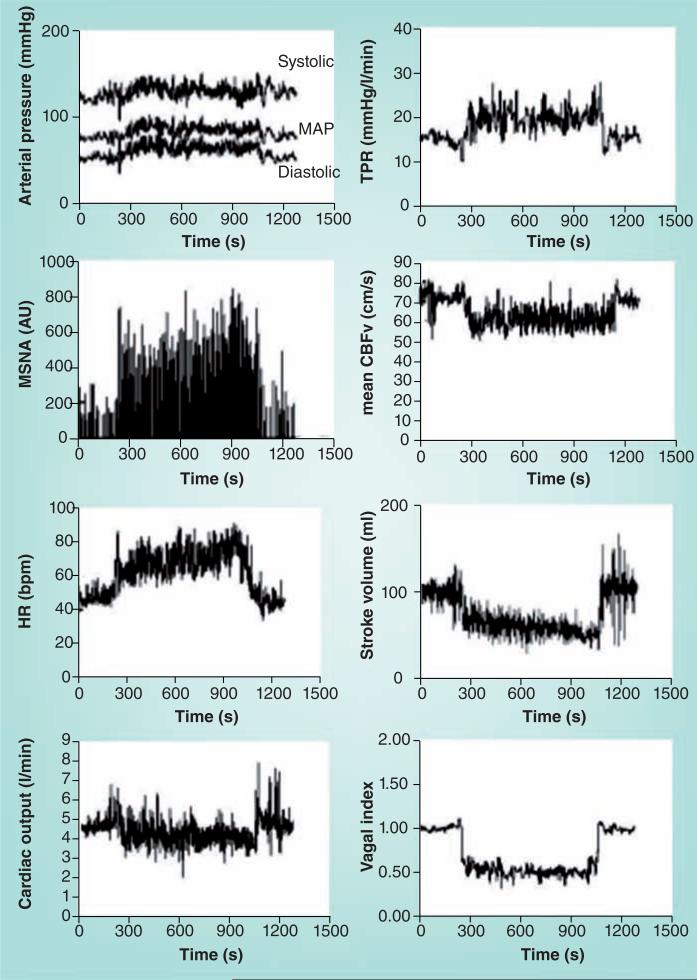
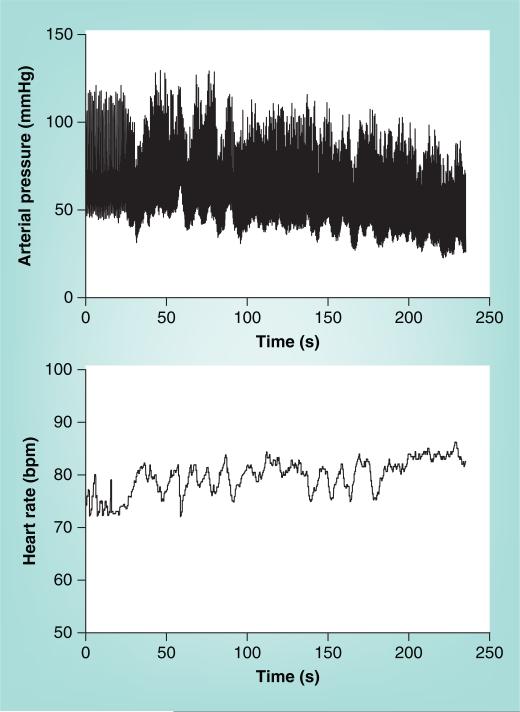
Orthostasis means standing upright. One speaks of orthostatic intolerance (OI) when signs, such as hypotension, and symptoms, such as lightheadedness, occur when upright and are relieved by recumbence. The experience of transient mild OI is part of daily life. 'Initial orthostatic hypotension' on rapid standing is a normal form of OI. However, other people experience OI that seriously interferes with quality of life. These include episodic acute OI, in the form of postural vasovagal syncope, and chronic OI, in the form of postural tachycardia syndrome. Less common is neurogenic orthostatic hypotension, which is an aspect of autonomic failure. Normal orthostatic physiology and potential mechanisms for OI are discussed, including forms of sympathetic hypofunction, forms of sympathetic hyperfunction and OI that results from regional blood volume redistribution. General and specific treatment options are proposed.
Figures
References
-
- Robertson D. The epidemic of orthostatic tachycardia and orthostatic intolerance. Am. J. Med. Sci. 1999;317(2):75–77. - PubMed
-
- LeLorier P, Klein GJ, Krahn A, Yee R, Skanes A, Shoemaker JK. Combined head-up tilt and lower body negative pressure as an experimental model of orthostatic syncope. J. Cardiovasc. Electrophysiol. 2003;14(9):920–924. - PubMed
-
- Low PA, Opfer-Gehrking TL, McPhee BR, et al. Prospective evaluation of clinical characteristics of orthostatic hypotension. Mayo Clin. Proc. 1995;70(7):617–622. - PubMed