

Neural and psychosocial contributions to sex differences in knee osteoarthritic pain
- PMID: 23244577
- PMCID: PMC3583673
- DOI: 10.1186/2042-6410-3-26
Neural and psychosocial contributions to sex differences in knee osteoarthritic pain
Abstract
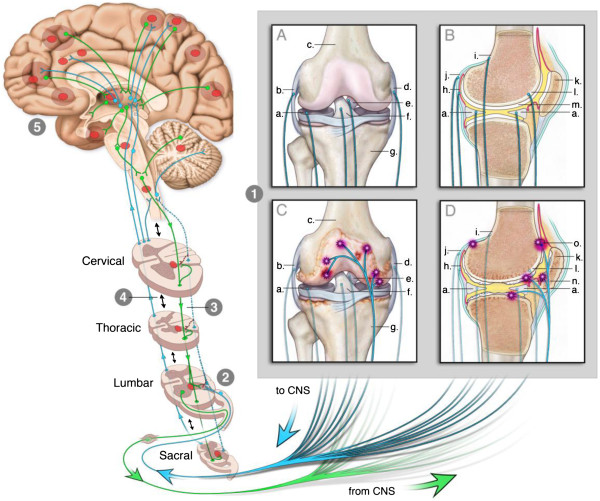
People with osteoarthritis (OA) can have significant pain that interferes with function and quality of life. Women with knee OA have greater pain and greater reductions in function and quality of life than men. In many cases, OA pain is directly related to sensitization and activation of nociceptors in the injured joint and correlates with the degree of joint effusion and synovial thickening. In some patients, however, the pain does not match the degree of injury and continues after removal of the nociceptors with a total joint replacement. Growth of new nociceptors, activation of nociceptors in the subchondral bone exposed after cartilage degradation, and nociceptors innervating synovium sensitized by inflammatory mediators could all augment the peripheral input to the central nervous system and result in pain. Enhanced central excitability and reduced central inhibition could lead to prolonged and enhanced pain that does not directly match the degree of injury. Psychosocial variables can influence pain and contribute to pain variability. This review explores the neural and psychosocial factors that contribute to knee OA pain with an emphasis on differences between the sexes and gaps in knowledge.
Figures

References
-
- Lethbridge-Cejku M, Scott WW Jr, Reichle R, Ettinger WH, Zonderman A, Costa P, Plato CC, Tobin JD, Hochberg MC. Association of radiographic features of osteoarthritis of the knee with knee pain: data from the Baltimore Longitudinal Study of Aging. Arthritis Care Res. 1995;8:182–188. doi: 10.1002/art.1790080311. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
