

Risk factors for dementia after critical illness in elderly Medicare beneficiaries
- PMID: 23245397
- PMCID: PMC3672622
- DOI: 10.1186/cc11901
Risk factors for dementia after critical illness in elderly Medicare beneficiaries
Abstract
Introduction: Hospitalization increases the risk of a subsequent diagnosis of dementia. We aimed to identify diagnoses or events during a hospitalization requiring critical care that are associated with a subsequent dementia diagnosis in the elderly.
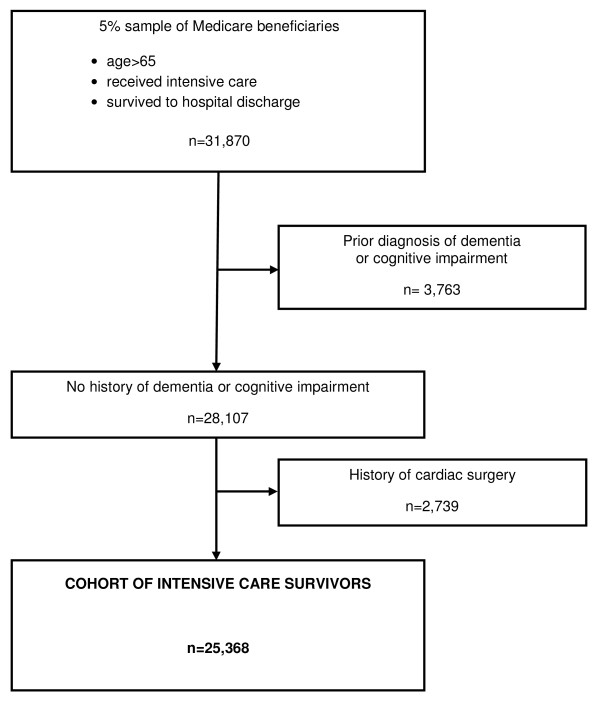
Methods: A cohort study of a random 5% sample of Medicare beneficiaries who received intensive care in 2005 and survived to hospital discharge, with three years of follow-up (through 2008) was conducted using Medicare claims files. We defined dementia using the International Classification of Diseases, 9th edition, clinical modification (ICD-9-CM) codes and excluded patients with any prior diagnosis of dementia or cognitive impairment in the year prior to admission. We used an extended Cox model to examine the association between diagnoses and events associated with the critical illness and a subsequent diagnosis of dementia, adjusting for known risk factors for dementia.
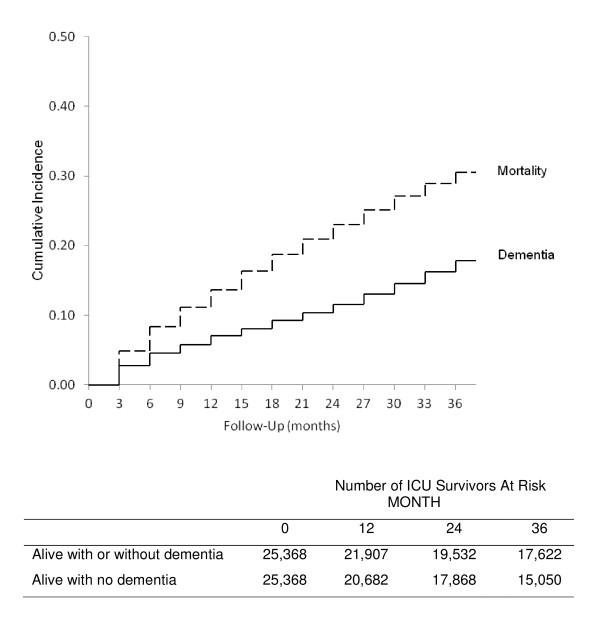
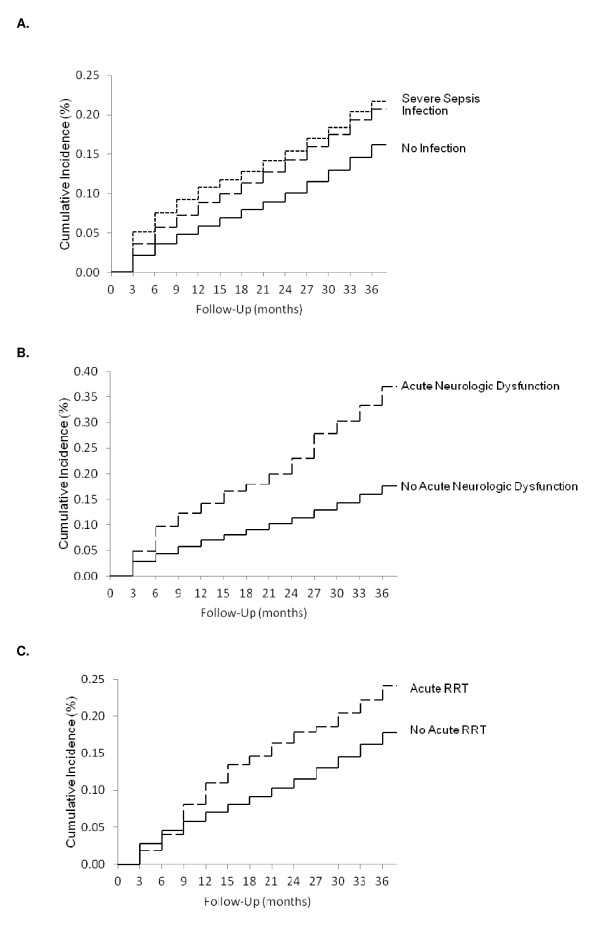
Results: Over the three years of follow-up, dementia was newly diagnosed in 4,519 (17.8%) of 25,368 patients who received intensive care and survived to hospital discharge. After accounting for known risk factors, having an infection (adjusted hazard ratio (AHR) = 1.25; 95% CI, 1.17 to 1.35), or a diagnosis of severe sepsis (AHR = 1.40; 95% CI, 1.28 to 1.53), acute neurologic dysfunction (AHR = 2.06; 95% CI, 1.72 to 2.46), and acute dialysis (AHR = 1.70; 95% CI, 1.30 to 2.23) were all independently associated with a subsequent diagnosis of dementia. No other measured ICU factors, such as need for mechanical ventilation, were independently associated.
Conclusions: Among ICU events, infection or severe sepsis, neurologic dysfunction, and acute dialysis were independently associated with a subsequent diagnosis of dementia. Patient prognostication, as well as future research into post-ICU cognitive decline, should focus on these higher-risk subgroups.
Figures
Comment in
-
The brain after critical illness: effect of illness and aging on cognitive function.Crit Care. 2013 Feb 6;17(1):116. doi: 10.1186/cc11913. Crit Care. 2013. PMID: 23384320 Free PMC article.
References
-
- Hopkins RO, Weaver LK, Pope D, Orme JF, Bigler ED, Larson LV. Neuropsychological sequelae and impaired health status in survivors of severe acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999;16:50–56. - PubMed
-
- Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados N, Al-Saidi F, Cooper AB, Guest CB, Mazer CD, Mehta S, Stewart TE, Barr A, Cook D, Slutsky AS. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003;16:683–693. doi: 10.1056/NEJMoa022450. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
