

Lateral soft tissue laxity increases but medial laxity does not contract with varus deformity in total knee arthroplasty
- PMID: 23247818
- PMCID: PMC3585995
- DOI: 10.1007/s11999-012-2745-1
Lateral soft tissue laxity increases but medial laxity does not contract with varus deformity in total knee arthroplasty
Abstract
Background: In TKA, soft tissue balance (the joint gap) depends on the amount of resected bone and soft tissue release. Some studies report preoperative bony deformity correlates with soft tissue balance evaluated intraoperatively and that the medial tissues are contracted with varus deformity. However, these studies did not take into account the amount of resected bone and did not describe whether the soft tissue was tight or loose. Therefore, it remains unclear whether in varus deformity the soft tissues on the medial side are contracted.
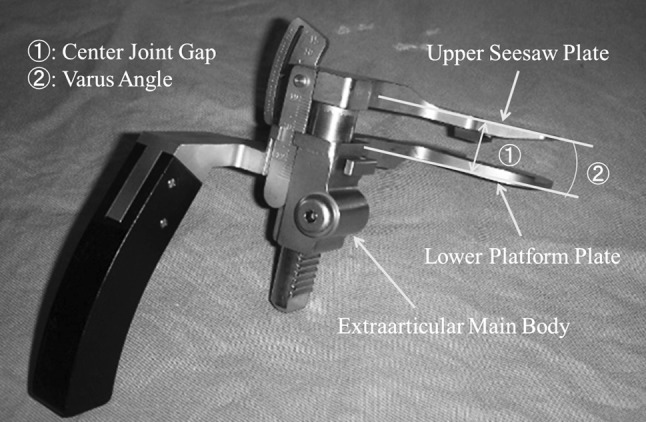
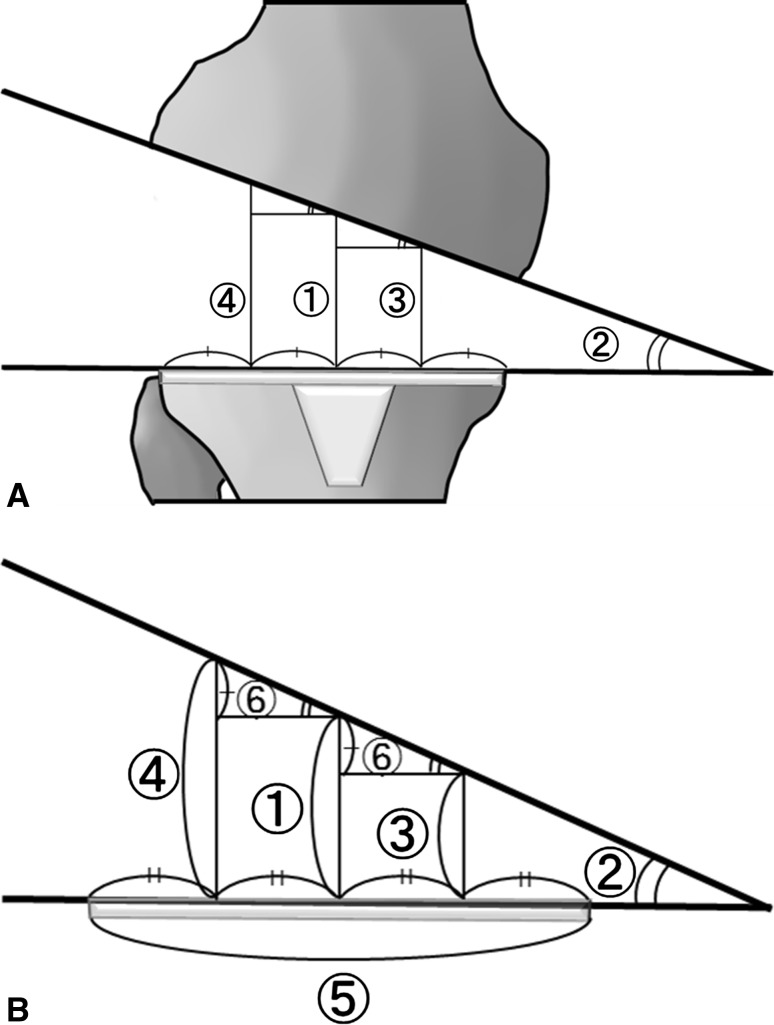
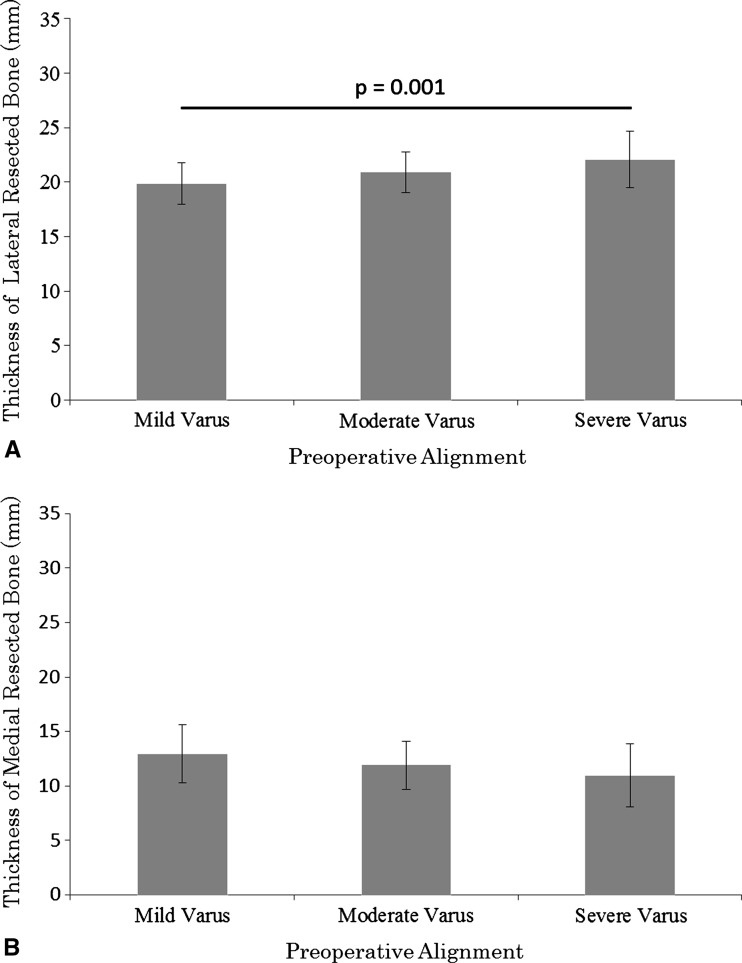
Questions/purposes: We compared (1) intraoperative joint gap, (2) amount of resected bone, and (3) intraoperative soft tissue laxity on the lateral and medial sides according to severity of preoperative varus deformity.
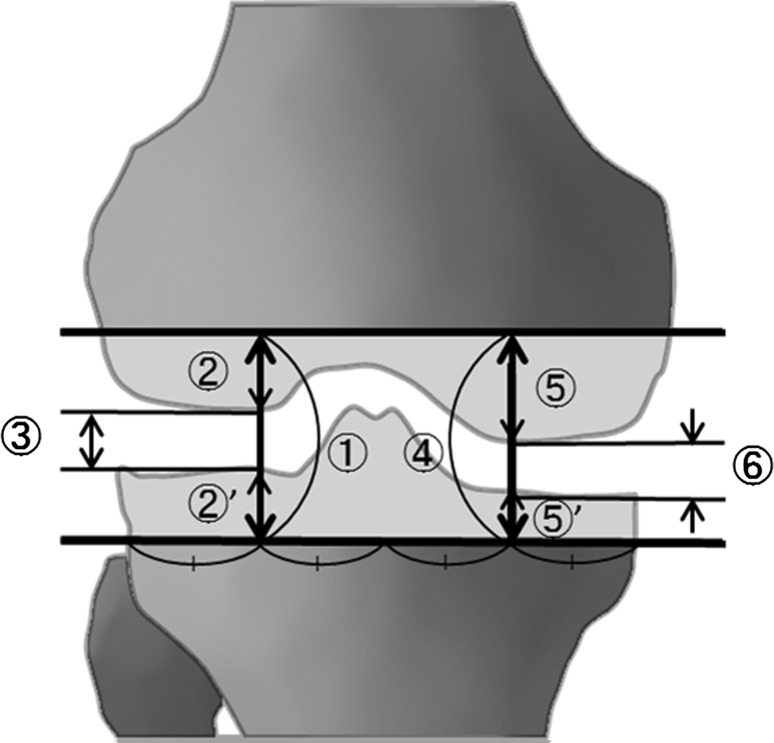
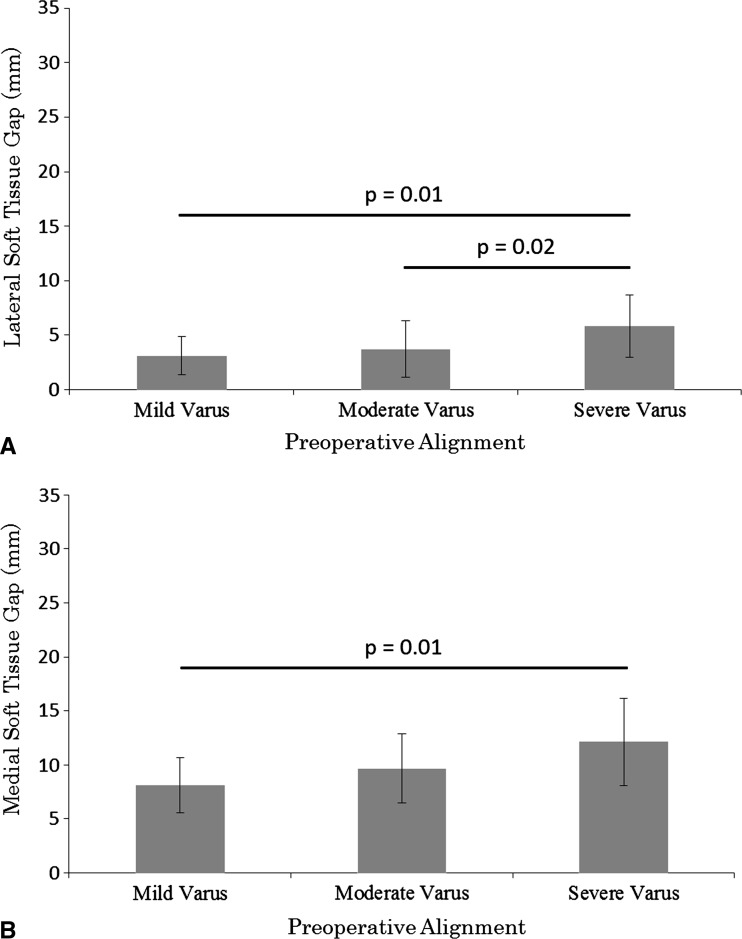
Methods: We retrospectively reviewed 70 patients with osteoarthritis and varus deformities who underwent 90 TKAs. We retrospectively divided the 90 knees into three groups according to degree of preoperative alignment: mild varus group (<10°), moderate varus group (10°-20°), and severe varus group (>20°). To evaluate intraoperative soft tissue tension, we calculated the soft tissue gap by subtracting the thickness of the resected bone from the joint gaps on the medial and lateral sides, respectively. We then explored the relationship between the soft tissue gap and preoperative alignment.
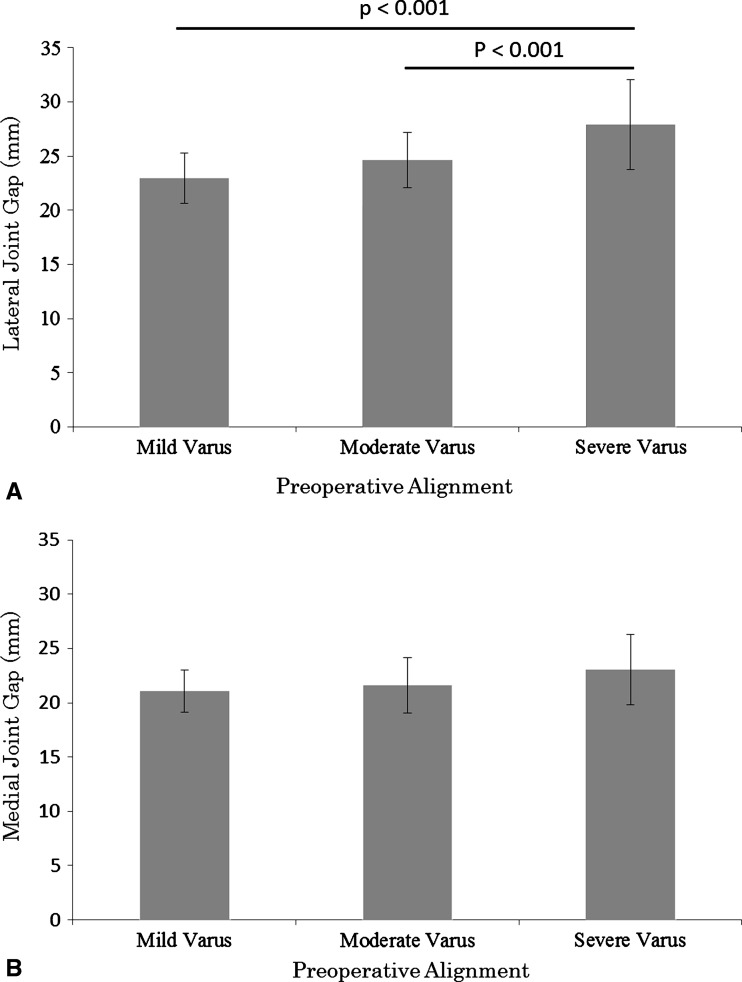
Results: The lateral soft tissue gap was larger in the severe varus group than in the mild and moderate varus groups. The medial soft tissue gap was larger in the severe varus group than in the mild varus group, but there were no differences in the medial joint gaps among the groups.
Conclusions: After the bone is resected, the soft tissue on the lateral side is more lax; however, the soft tissue on the medial side is not shorter with greater preoperative varus deformity.
Figures
References
-
- Brage ME, Draganich LF, Pottenger LA, Curran JJ. Knee laxity in symptomatic osteoarthritis. Clin Orthop Relat Res. 1994;304:184–189. - PubMed
-
- Brooks P. Seven cuts to the perfect total knee. Orthopedics. 2009;32. pii: orthosupersite.com/view.asp?rID = 42848. DOI: 10.3928/01477447-20090728-27. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
