

Exercise-induced wheeze, urgent medical visits, and neighborhood asthma prevalence
- PMID: 23248227
- PMCID: PMC3529949
- DOI: 10.1542/peds.2012-1072
Exercise-induced wheeze, urgent medical visits, and neighborhood asthma prevalence
Abstract
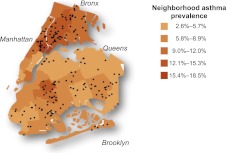
Objective: Exercise-induced wheeze (EIW) may identify a distinct population among asthmatics and give insight into asthma morbidity etiology. The prevalence of pediatric asthma and associated urgent medical visits varies greatly by neighborhood in New York City and is highest in low-income neighborhoods. Although increased asthma severity might contribute to the disparities in urgent medical visits, when controlling for health insurance coverage, we previously observed no differences in clinical measures of severity between asthmatic children living in neighborhoods with lower (3%-9%) versus higher (11%-19%) asthma prevalence. Among these asthmatics, we hypothesized that EIW would be associated with urgent medical visits and a child's neighborhood asthma prevalence.
Methods: Families of 7- to 8-year-old children were recruited into a case-control study of asthma through an employer-based health insurance provider. Among the asthmatics (n = 195), prevalence ratios (PRs) for EIW were estimated. Final models included children with valid measures of lung function, seroatopy, and waist circumference (n = 140).
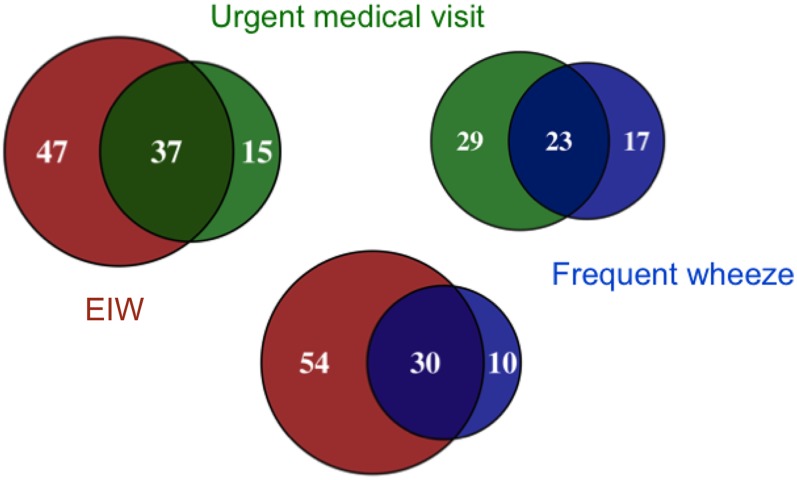
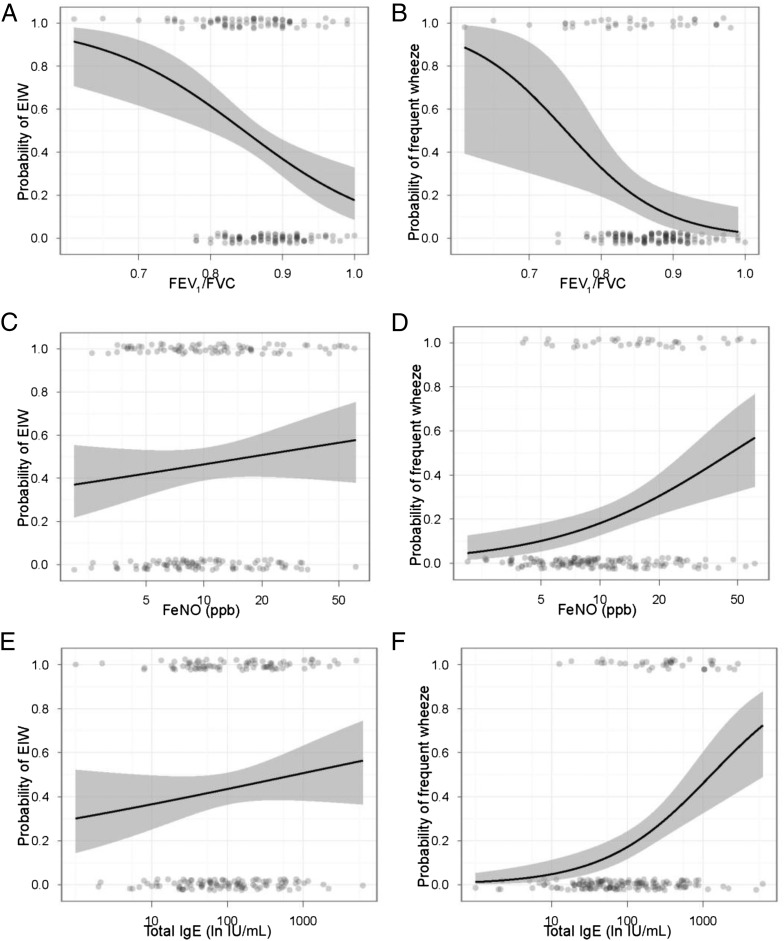
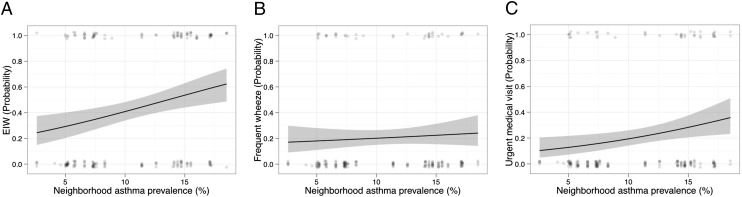
Results: EIW was associated with urgent medical visits for asthma (PR, 2.29; P = .021), independent of frequent wheeze symptoms. In contrast to frequent wheeze, EIW was not associated with seroatopy or exhaled NO, suggesting a distinct mechanism. EIW prevalence among asthmatics increased with increasing neighborhood asthma prevalence (PR, 1.09; P = .012), after adjustment for race, ethnicity, maternal asthma, environmental tobacco smoke, household income, and neighborhood income.
Conclusions: EIW may contribute to the disparities in urgent medical visits for asthma between high- and low-income neighborhoods. Physicians caring for asthmatics should consider EIW an indicator of risk for urgent medical visits.
Figures
References
-
- Martinez FD. Development of wheezing disorders and asthma in preschool children. Pediatrics. 2002;109(suppl 2):362–367 - PubMed
-
- Lötvall J, Akdis CA, Bacharier LB, et al. . Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome. J Allergy Clin Immunol. 2011;127(2):355–360 - PubMed
-
- McFadden ER, Jr, Gilbert IA. Exercise-induced asthma. N Engl J Med. 1994;330(19):1362–1367 - PubMed
-
- Hallstrand TS, Henderson WR, Jr. Role of leukotrienes in exercise-induced bronchoconstriction. Curr Allergy Asthma Rep. 2009;9(1):18–25 - PubMed
-
- Anderson SD, Kippelen P. Airway injury as a mechanism for exercise-induced bronchoconstriction in elite athletes. J Allergy Clin Immunol. 2008;122(2):225–235, quiz 236–237 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
