

Non-specific, functional, and somatoform bodily complaints
- PMID: 23248710
- PMCID: PMC3521192
- DOI: 10.3238/arztebl.2012.0803
Non-specific, functional, and somatoform bodily complaints
Abstract
Background: 4-10% of the general population and 20% of primary care patients have what are called "non-specific, functional, and somatoform bodily complaints." These often take a chronic course, markedly impair the sufferers' quality of life, and give rise to high costs. They can be made worse by inappropriate behavior on the physician's part.
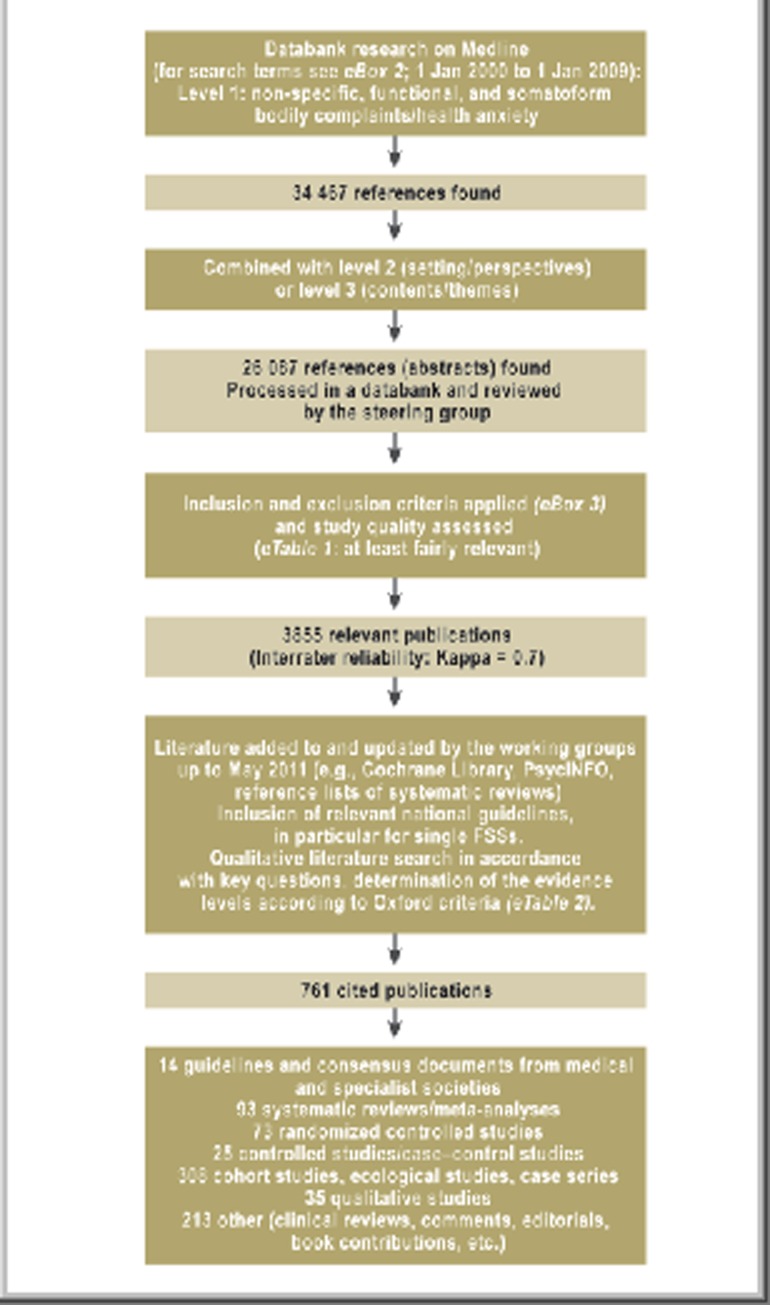
Methods: The new S3 guideline was formulated by representatives of 29 medical and psychological specialty societies and one patient representative. They analyzed more than 4000 publications retrieved by a systematic literature search and held two online Delphi rounds and three consensus conferences.
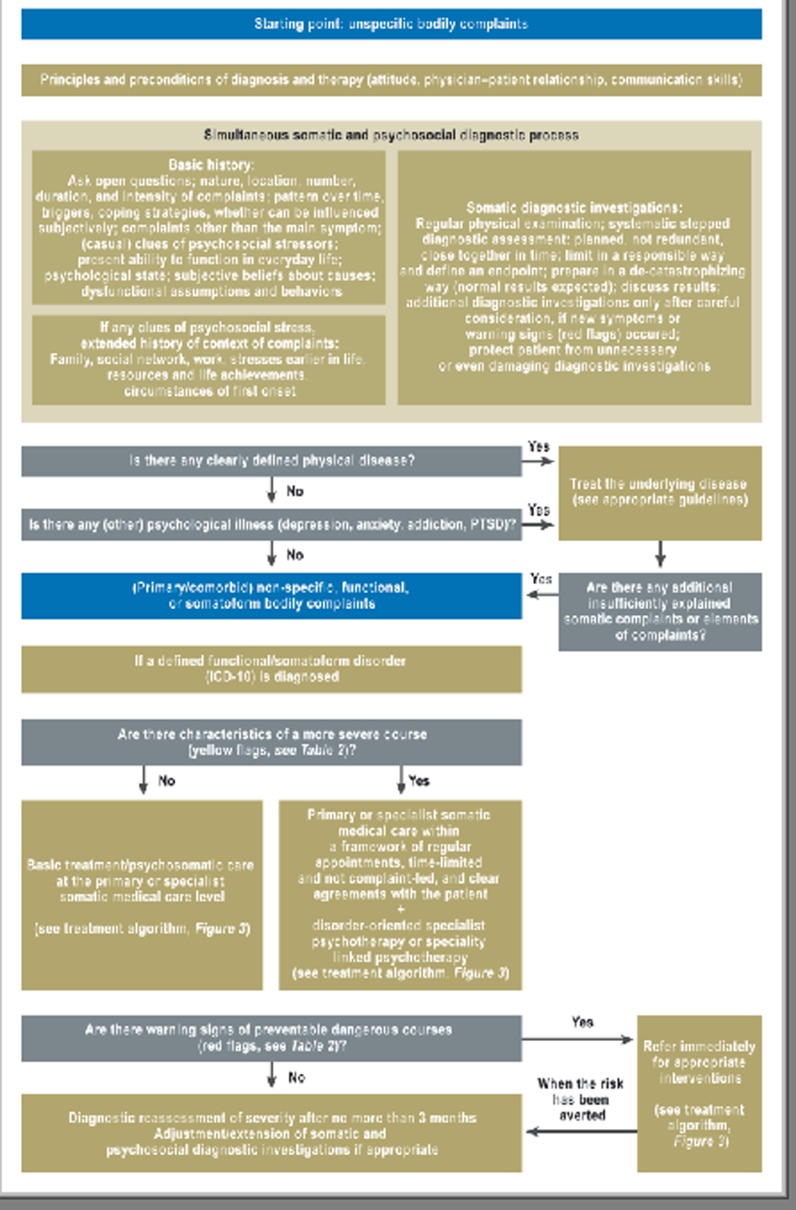
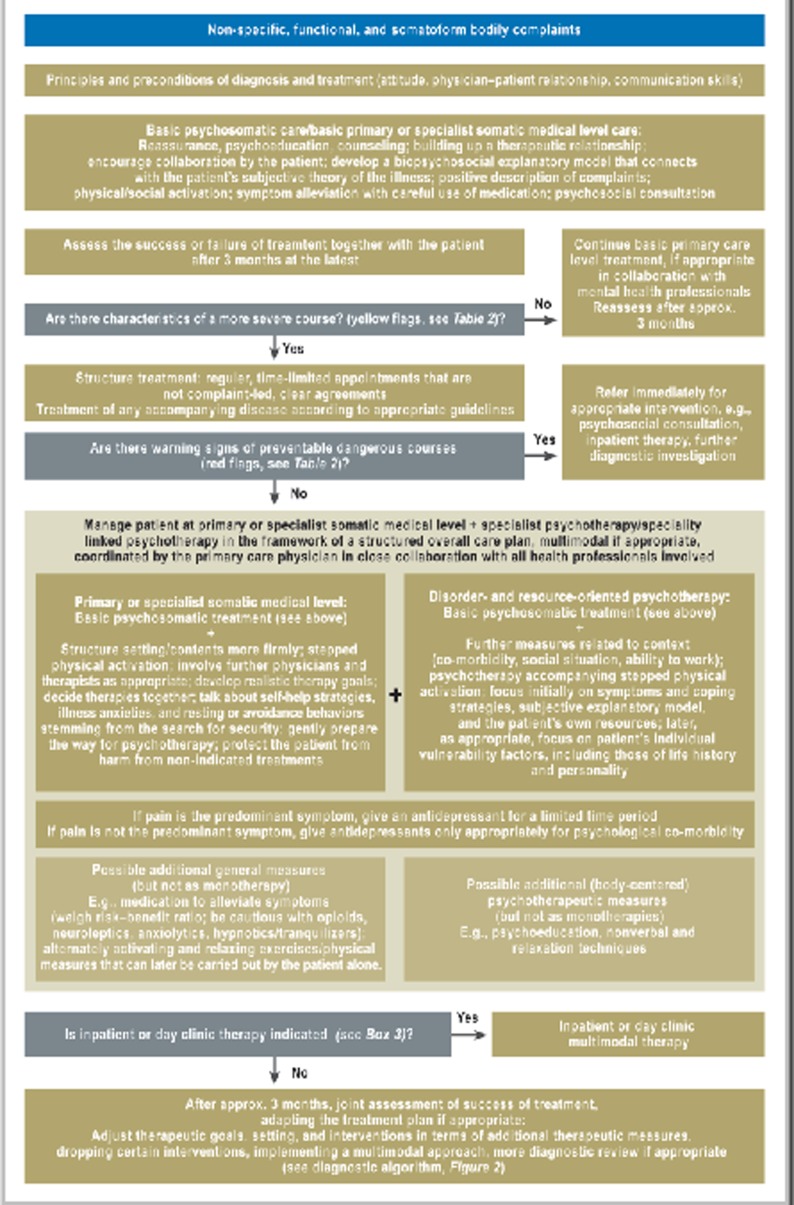
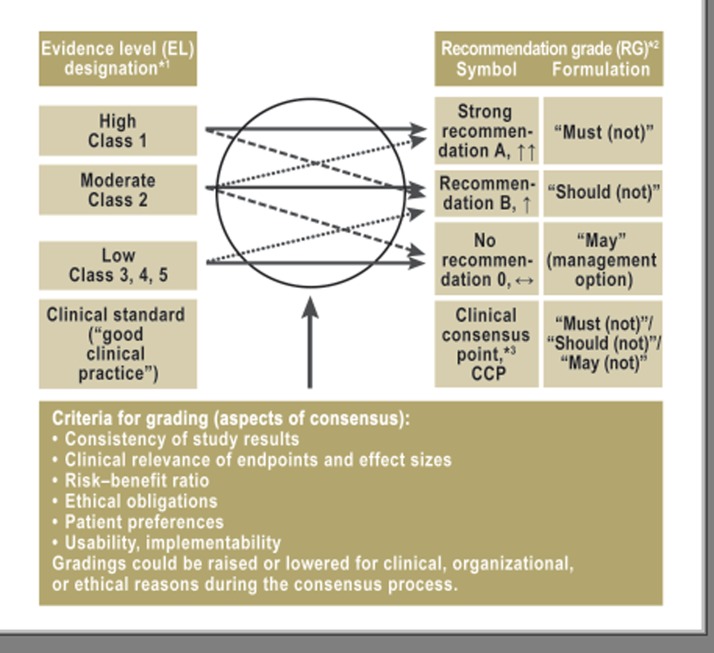
Results: Because of the breadth of the topic, the available evidence varied in quality depending on the particular subject addressed and was often only of moderate quality. A strong consensus was reached on most subjects. In the new guideline, it is recommended that physicians should establish a therapeutic alliance with the patient, adopt a symptom/coping-oriented attitude, and avoid stigmatizing comments. A biopsychosocial diagnostic evaluation, combined with sensitive discussion of signs of psychosocial stress, enables the early recognition of problems of this type, as well as of comorbid conditions, while lowering the risk of iatrogenic somatization. For mild, uncomplicated courses, the establishment of a biopsychosocial explanatory model and physical/social activation are recommended. More severe, complicated courses call for collaborative, coordinated management, including regular appointments (as opposed to ad-hoc appointments whenever the patient feels worse), graded activation, and psychotherapy; the latter may involve cognitive behavioral therapy or a psychodynamic-interpersonal or hypnotherapeutic/imaginative approach. The comprehensive treatment plan may be multimodal, potentially including body-oriented/non-verbal therapies, relaxation training, and time-limited pharmacotherapy.
Conclusion: A thorough, simultaneous biopsychosocial diagnostic assessment enables the early recognition of non-specific, functional, and somatoform bodily complaints. The appropriate treatment depends on the severity of the condition. Effective treatment requires the patient's active cooperation and the collaboration of all treating health professionals under the overall management of the patient's primary-care physician.
Figures
Comment in
-
Iatrogenic chronification as a result of pseudo diagnosis.Dtsch Arztebl Int. 2013 Apr;110(15):270. doi: 10.3238/arztebl.2013.0270a. Dtsch Arztebl Int. 2013. PMID: 23667396 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2013 Apr;110(15):270. doi: 10.3238/arztebl.2013.0270b. Dtsch Arztebl Int. 2013. PMID: 23667397 Free PMC article. No abstract available.
References
-
- Henningsen P, Hartkamp N, Loew T, Sack M, Scheidt CE, Rudolf G. Somatoforme Störungen. Leitlinien und Quellentexte. Schattauer. 2002
-
- Hausteiner-Wiehle C, Schaefert R, Sattel H, Ronel J, Herrmann M, Häuser W, Henningsen P. AWMF-Leitlinie zum Umgang mit Patienten mit nicht-spezifischen, funktionellen und somatoformen Körperbeschwerden AWMF-Reg.-Nr. 051-001 2012. www.awmf.org/leitlinien/detail/ll/051-001.html. 2012 Sep 16; last accessed on. - PubMed
-
- Hausteiner-Wiehle C, Schaefert R, Sattel H, Ronel J, Herrmann M, Häuser W, Henningsen P. AWMF-Leitlinie zum Umgang mit Patienten mit nicht-spezifischen, funktionellen und somatoformen Körperbeschwerden - Leitlinienreport AWMF-Reg.-Nr. 051-001 2012. http://www.awmf.org/leitlinien/detail/ll/051-001.html. 2012 Sep 16; last accessed on. - PubMed
-
- Hausteiner-Wiehle C, Henningsen P, Häuser W, Herrmann M, Ronel J, Sattel H, Schäfert R. Schattauer. Stuttgart: in press; 2012. Umgang mit Patienten mit nicht-spezifischen, funktionellen und somatoformen Körperbeschwerden. S3-Leitlinien mit Quellentexten und Praxismaterialien. - PubMed
-
- Layer P, Andresen V, Pehl C, Allescher H, Bischoff SC, Classen M, et al. S3-Leitlinie Reizdarmsyndrom: Definition, Pathophysiologie, Diagnostik und Therapie Gemeinsame. Leitlinie der Deutschen Gesellschaft für Verdauungs- und Stoffwechselkrankheiten (DGVS) und der Deutschen Gesellschaft für Neurogastroenterologie und Motilität (DGNM) [Irritable Bowel Syndrome: German Consensus Guidelines on Definition, Pathophysiology and Management. German Society of Digestive and Metabolic Diseases (DGVS) and German Society of Neurogastroenterology and Motility (DGNM)] Z Gastroenterol. 2011;49:237–293. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous