

A brief review of chronic obstructive pulmonary disease
- PMID: 23248802
- PMCID: PMC3603763
- DOI: 10.1155/2012/496563
A brief review of chronic obstructive pulmonary disease
Abstract
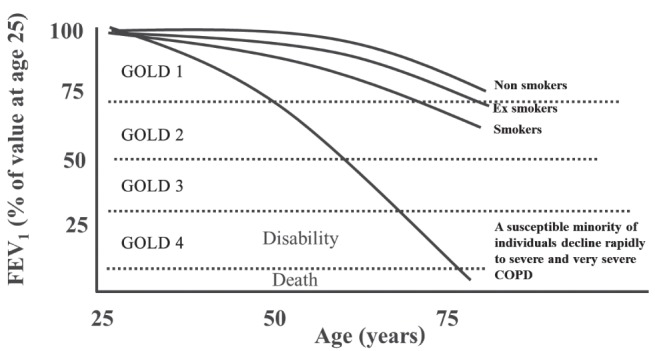
A recent study, based on a combination of multidetector computed tomography scanning of an intact specimen with microcomputed tomography and histological analysis of lung tissue samples, reported that the number of terminal bronchioles were reduced from approximately 44,500/lung pair in control (donor) lungs to approximately 4800/lung pair in lungs donated by individuals with very severe (Global initiative for chronic Obstructive Lung Disease stage 4) chronic obstructive pulmonary disease (COPD) treated by lung transplantation. The present short review discusses the hypothesis that a rapid rate of terminal bronchiolar destruction causes the rapid decline in lung function leading to advanced COPD. With respect to why the terminal bronchioles are targeted for destruction, the postulated mechanisms of this destruction and the possibility that new treatments are able to either prevent or reverse the underlying cause of airway obstruction in COPD are addressed.
Une récente étude, fondée sur une association de tomographie assistée par ordinateur à détecteurs multiples d’un spécimen intact et d’une tomographie assistée par ordinateur avec l’analyse histologique d’échantillons de tissus pulmonaires, a établi que le nombre de bronchioles terminales avait fléchi d’environ 44 500 par paire de poumons chez les sujets témoins (donneurs) à environ 4 800 par paire de poumons chez les personnes ayant une très grave maladie pulmonaire obstructive chronique (MPOC) (phase 4 selon la Global initiative for chronic Obstructive Lung Disease) traitée par greffe pulmonaire. La présente brève analyse porte sur l’hypothèse selon laquelle un taux rapide de destruction des bronchioles terminales provoque le rapide déclin de la fonction pulmonaire, menant à une MPOC avancée. Pour ce qui est des raisons pour lesquelles les bronchioles terminales sont ciblées, les chercheurs exposent les mécanismes postulés de leur destruction et la possibilité que de nouveaux traitements puissent prévenir ou renverser la cause sous-jacente de l’obstruction des voies aériennes en cas de MPOC.
Figures
Similar articles
-
Small airways disease in mild and moderate chronic obstructive pulmonary disease: a cross-sectional study.Lancet Respir Med. 2018 Aug;6(8):591-602. doi: 10.1016/S2213-2600(18)30196-6. Epub 2018 Jul 4. Lancet Respir Med. 2018. PMID: 30072106
-
Analysis of airway pathology in COPD using a combination of computed tomography, micro-computed tomography and histology.Eur Respir J. 2018 Feb 14;51(2):1701245. doi: 10.1183/13993003.01245-2017. Print 2018 Feb. Eur Respir J. 2018. PMID: 29444912 Free PMC article.
-
What drives the peripheral lung-remodeling process in chronic obstructive pulmonary disease?Proc Am Thorac Soc. 2009 Dec;6(8):668-72. doi: 10.1513/pats.200907-079DP. Proc Am Thorac Soc. 2009. PMID: 20008873 Free PMC article. Review.
-
Small airway obstruction in COPD: new insights based on micro-CT imaging and MRI imaging.Chest. 2013 May;143(5):1436-1443. doi: 10.1378/chest.12-1766. Chest. 2013. PMID: 23648907 Free PMC article. Review.
-
The molecular and cellular mechanisms associated with the destruction of terminal bronchioles in COPD.Eur Respir J. 2022 May 26;59(5):2101411. doi: 10.1183/13993003.01411-2021. Print 2022 May. Eur Respir J. 2022. PMID: 34675046
Cited by
-
High levels of biomarkers of collagen remodeling are associated with increased mortality in COPD - results from the ECLIPSE study.Respir Res. 2016 Oct 4;17(1):125. doi: 10.1186/s12931-016-0440-6. Respir Res. 2016. PMID: 27716343 Free PMC article.
-
Host-Derived Cytotoxic Agents in Chronic Inflammation and Disease Progression.Int J Mol Sci. 2023 Feb 3;24(3):3016. doi: 10.3390/ijms24033016. Int J Mol Sci. 2023. PMID: 36769331 Free PMC article. Review.
-
Club Cell Secreted Protein CC16: Potential Applications in Prognosis and Therapy for Pulmonary Diseases.J Clin Med. 2020 Dec 14;9(12):4039. doi: 10.3390/jcm9124039. J Clin Med. 2020. PMID: 33327505 Free PMC article. Review.
-
The Lung Immune Response to Nontypeable Haemophilus influenzae (Lung Immunity to NTHi).J Immunol Res. 2015;2015:706376. doi: 10.1155/2015/706376. Epub 2015 May 31. J Immunol Res. 2015. PMID: 26114124 Free PMC article. Review.
-
Dynamic airway function during exercise in COPD assessed via impulse oscillometry before and after inhaled bronchodilators.J Appl Physiol (1985). 2021 Jul 1;131(1):326-338. doi: 10.1152/japplphysiol.00148.2021. Epub 2021 May 20. J Appl Physiol (1985). 2021. PMID: 34013748 Free PMC article.
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (updated 2009) < www.goldcopd.org> (Accessed May 31, 2012). - PubMed
-
- Buist AS, McBurnie MA, Vollmer WM, et al. Bold study of the prevalence of obstructive lung disease International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet. 2007;370:741–50. - PubMed
-
- Weibel ER. Morphometry of the Human Lung. New York: Academic Press Inc; 1963.
-
- Green M. How big are the bronchioles? St Thomas Hospital Gazette. 1965;63:136–9.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
