

Craniosynostosis: molecular pathways and future pharmacologic therapy
- PMID: 23249483
- PMCID: PMC3562251
- DOI: 10.4161/org.23307
Craniosynostosis: molecular pathways and future pharmacologic therapy
Abstract
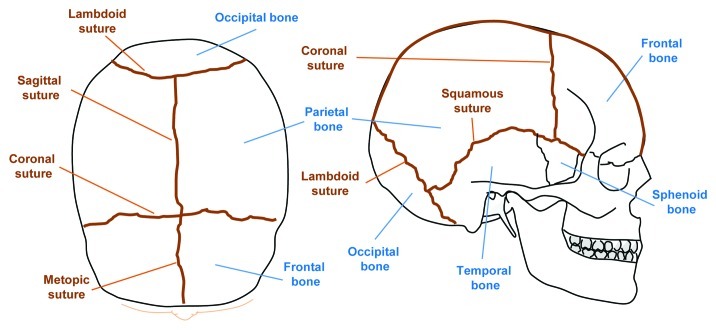
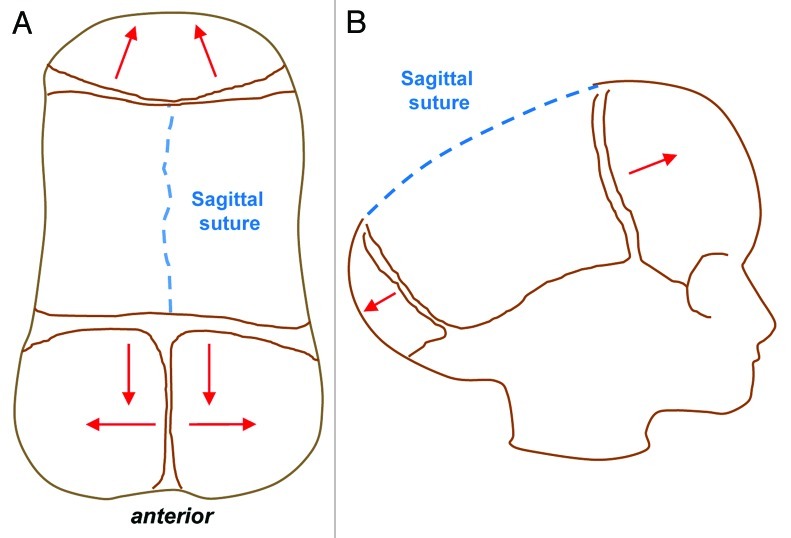
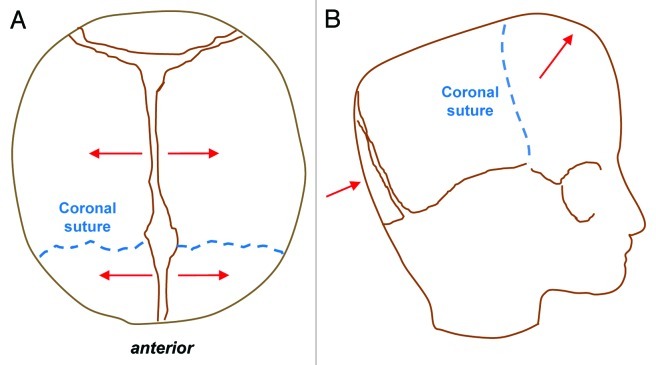
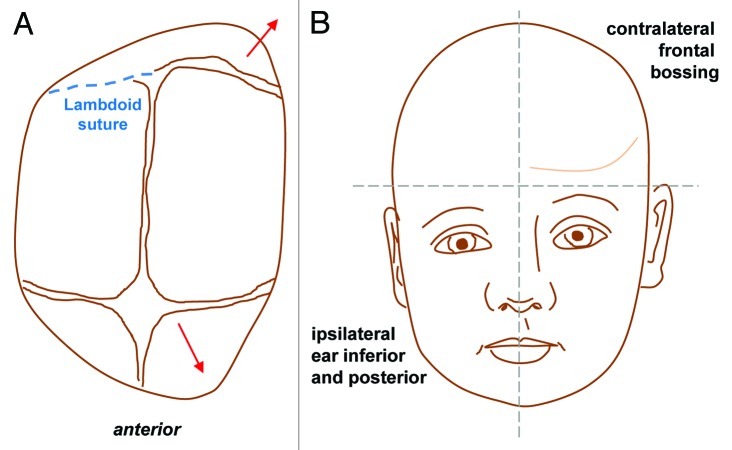
Craniosynostosis describes the premature fusion of one or more cranial sutures and can lead to dramatic manifestations in terms of appearance and functional impairment. Contemporary approaches for this condition are primarily surgical and are associated with considerable morbidity and mortality. The additional post-operative problems of suture refusion and bony relapse may also necessitate repeated surgeries with their own attendant risks. Therefore, a need exists to not only optimize current strategies but also to develop novel biological therapies which could obviate the need for surgery and potentially treat or even prevent premature suture fusion. Clinical studies of patients with syndromic craniosynostosis have provided some useful insights into the important signaling pathways and molecular events guiding suture fate. Furthermore, the highly conserved nature of craniofacial development between humans and other species have permitted more focused and step-wise elucidation of the molecular underpinnings of craniosynostosis. This review will describe the clinical manifestations of craniosynostosis, reflect on our understanding of syndromic and non-syndromic craniosynostoses and outline the different approaches that have been adopted in our laboratory and elsewhere to better understand the pathogenesis of premature suture fusion. Finally, we will assess to what extent our improved understanding of the pathogenesis of craniosynostosis, achieved through laboratory-based and clinical studies, have made the possibility of a non-surgical pharmacological approach both realistic and tangible.
Keywords: FGF; calvarium; craniosynostosis; signaling; suture.
Figures

References
-
- Otto. A. Lehrbuch der Pathologischen Anatomie. Berlin, Germany: Rucher., 1830.
-
- Virchow R. Berh Phyd Med Gesellsch Wuerzburg. 1851;2:231–71.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources