

In vivo detection of cerebral cortical microinfarcts with high-resolution 7T MRI
- PMID: 23250109
- PMCID: PMC3587820
- DOI: 10.1038/jcbfm.2012.196
In vivo detection of cerebral cortical microinfarcts with high-resolution 7T MRI
Abstract
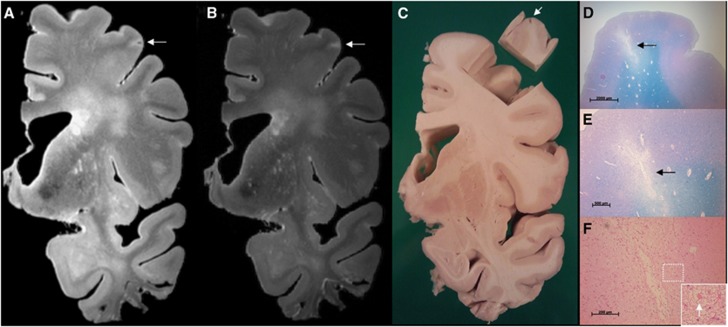
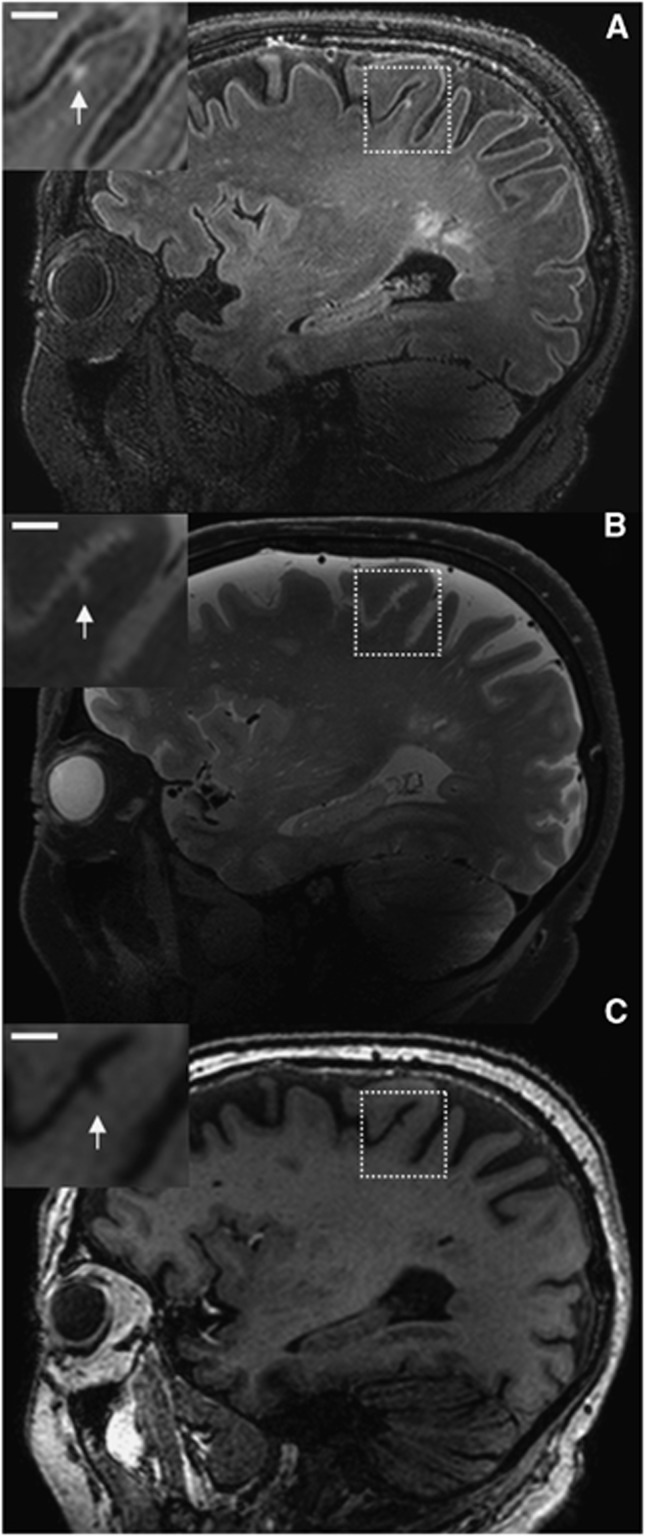
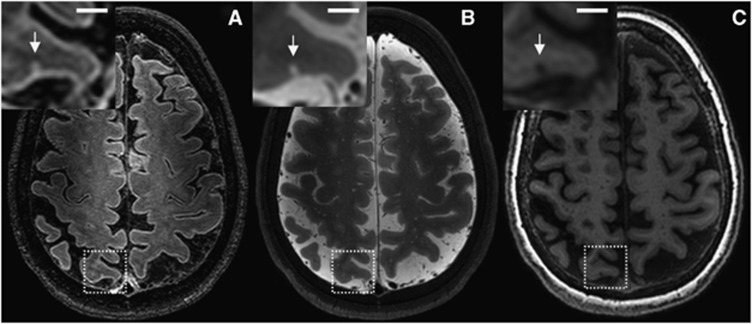
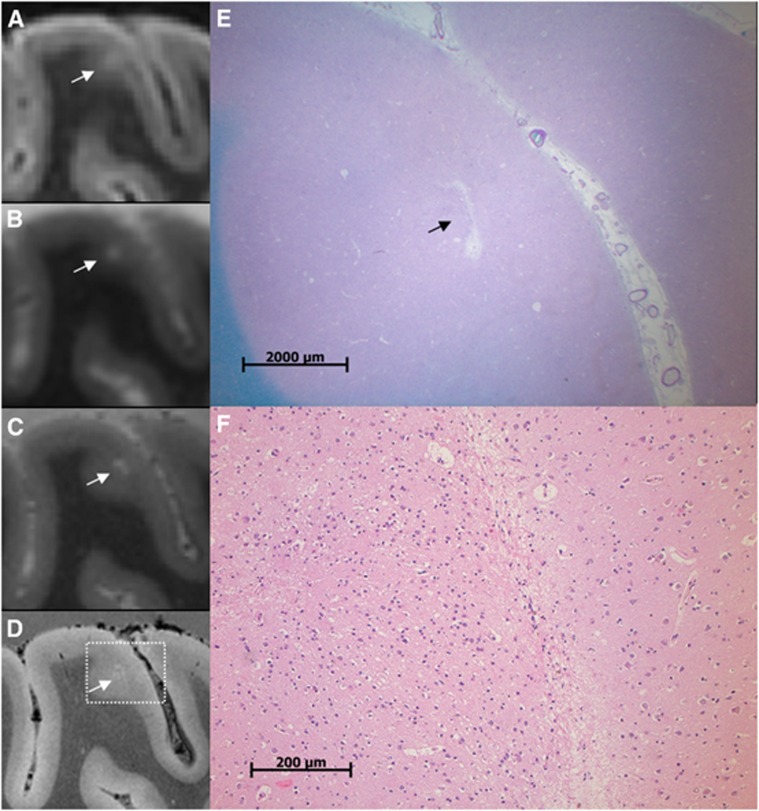
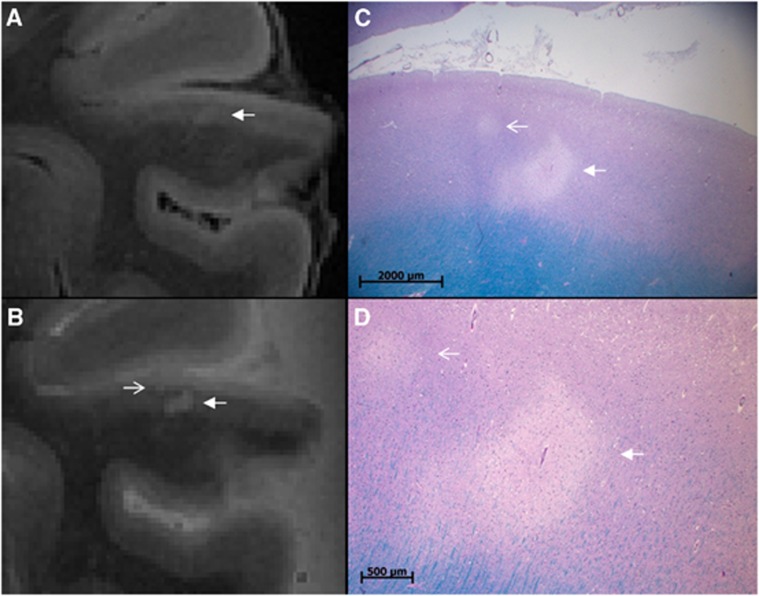
Cerebrovascular disease has an important role in cognitive decline and dementia. In this context, cerebral microinfarcts are attracting increasing attention, but these lesions could thus far not be detected in vivo. The aim of this study was to try to identify possible cortical microinfarcts on high-resolution 7T in vivo magnetic resonance imaging (MRI) and to perform a histopathologic validation study on similar appearing lesions on 7T ex vivo MRI of postmortem brain tissue. The study population consisted of 22 elderly subjects, who underwent 7T MRI. The fluid attenuated inversion recovery, T(2), and T(1) weighted scans of these subjects were examined for possible cortical microinfarcts. In the ex vivo MRI study, 15 formalin-fixed coronal brain slices of 6 subjects with Alzheimer and vascular pathology were examined and subjected to histopathologic verification. On the in vivo scans, 15 cortical lesions could be identified that were likely to be microinfarcts in 6 subjects. In the postmortem tissue, 6 similar appearing lesions were identified of which 5 were verified as cortical microinfarcts on histopathology. This study provides strong evidence that cortical microinfarcts can be detected in vivo, which will be of great value in further studies into the role of vascular disease in cognitive decline and dementia.
Figures
Comment in
-
New insights into vascular pathology by ultrahigh-field magnetic resonance imaging.J Cereb Blood Flow Metab. 2013 Mar;33(3):321. doi: 10.1038/jcbfm.2012.197. Epub 2012 Dec 19. J Cereb Blood Flow Metab. 2013. PMID: 23250104 Free PMC article. No abstract available.
References
-
- Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol. 2009;8:1006–1018. - PubMed
-
- Kalaria RN, Kenny RA, Ballard CG, Perry R, Ince P, Polvikoski T. Towards defining the neuropathological substrates of vascular dementia. J Neurol Sci. 2004;226:75–80. - PubMed
-
- Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology. 2007;69:2197–2204. - PubMed
-
- Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010;9:689–701. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
