

Survival trends in pediatric in-hospital cardiac arrests: an analysis from Get With the Guidelines-Resuscitation
- PMID: 23250980
- PMCID: PMC3555689
- DOI: 10.1161/CIRCOUTCOMES.112.967968
Survival trends in pediatric in-hospital cardiac arrests: an analysis from Get With the Guidelines-Resuscitation
Abstract
Background: Despite ongoing efforts to improve the quality of pediatric resuscitation, it remains unknown whether survival in children with in-hospital cardiac arrest has improved.
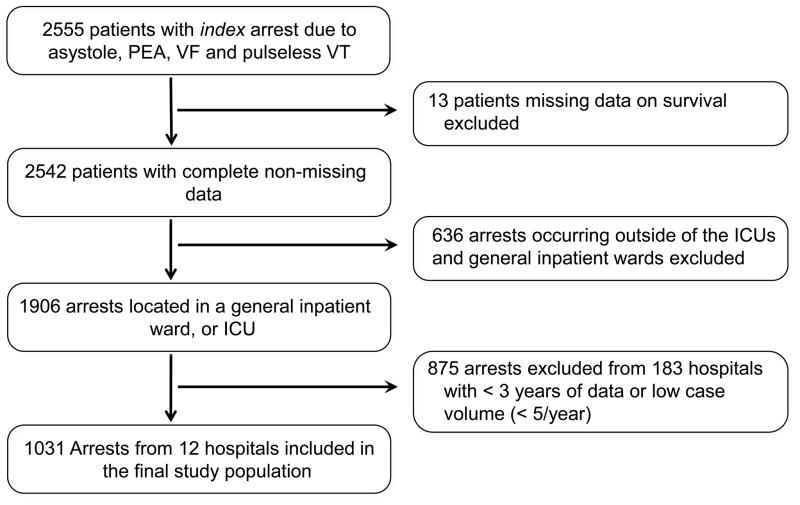
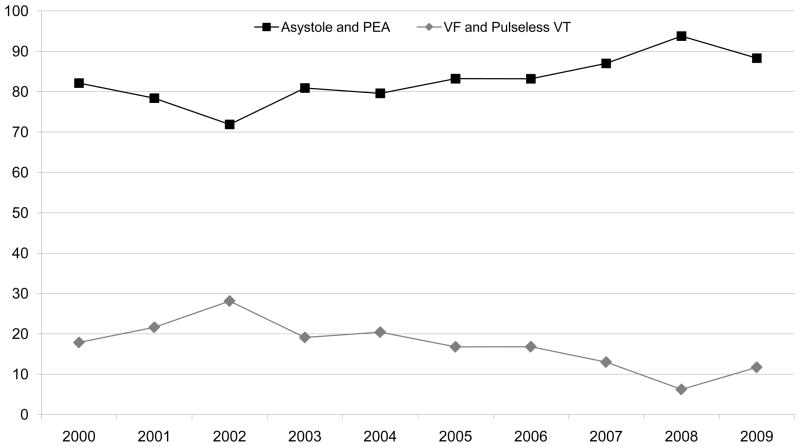
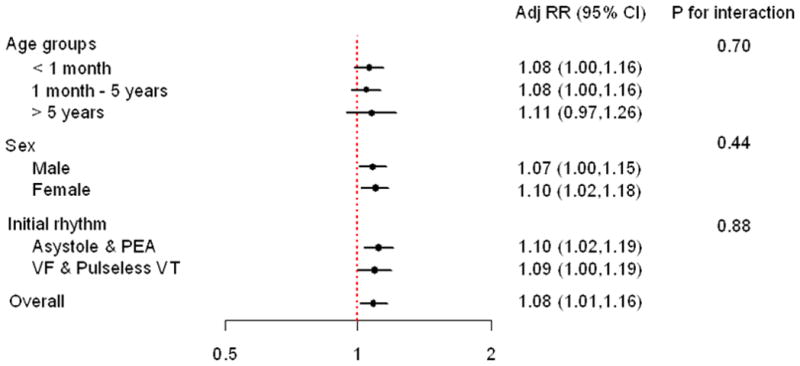
Methods and results: Between 2000 and 2009, we identified children (<18 years of age) with an in-hospital cardiac arrest at hospitals with >3 years of participation and >5 cases annually within the national Get With The Guidelines-Resuscitation registry. Multivariable logistic regression was used to examine temporal trends in survival to discharge. We also explored whether trends in survival were attributable to improvement in acute resuscitation or postresuscitation care and examined trends in neurological disability among survivors. Among 1031 children at 12 hospitals, the initial cardiac arrest rhythm was asystole and pulseless electrical activity in 874 children (84.8%) and ventricular fibrillation and pulseless ventricular tachycardia in 157 children (15.2%), with an increase in cardiac arrests due to pulseless electrical activity over time (P for trend <0.001). Risk-adjusted rates of survival to discharge increased from 14.3% in 2000 to 43.4% in 2009 (adjusted rate ratio per year, 1.08; 95% confidence interval, 1.01-1.16; P for trend=0.02). Improvement in survival was driven largely by an improvement in acute resuscitation survival (risk-adjusted rates: 42.9% in 2000, 81.2% in 2009; adjusted rate ratio per year: 1.04; 95% confidence interval, 1.01-1.08; P for trend=0.006). Moreover, survival trends were not accompanied by higher rates of neurological disability among survivors over time (unadjusted P for trend=0.32), suggesting an overall increase in the number of survivors without neurological disability over time.
Conclusions: Rates of survival to hospital discharge in children with in-hospital cardiac arrests have improved over the past decade without higher rates of neurological disability among survivors.
Figures
References
-
- Suominen P, Olkkola KT, Voipio V, Korpela R, Palo R, Rasanen J. Utstein style reporting of in-hospital paediatric cardiopulmonary resuscitation. Resuscitation. 2000;45:17–25. - PubMed
-
- Reis AG, Nadkarni V, Perondi MB, Grisi S, Berg RA. A prospective investigation into the epidemiology of in-hospital pediatric cardiopulmonary resuscitation using the international Utstein reporting style. Pediatrics. 2002;109:200–209. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, Carey SM, Kaye W, Mancini ME, Nichol G, Lane-Truitt T, Potts J, Ornato JP, Berg RA. First documented rhythm and clinical outcome from inhospital cardiac arrest among children and adults. JAMA. 2006;295:50–57. - PubMed
-
- de Mos N, van Litsenburg RR, McCrindle B, Bohn DJ, Parshuram CS. Pediatric in-intensive-care-unit cardiac arrest: incidence, survival, and predictive factors. Crit Care Med. 2006;34:1209–1215. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
