

Markers of decongestion, dyspnea relief, and clinical outcomes among patients hospitalized with acute heart failure
- PMID: 23250981
- PMCID: PMC3865520
- DOI: 10.1161/CIRCHEARTFAILURE.112.969246
Markers of decongestion, dyspnea relief, and clinical outcomes among patients hospitalized with acute heart failure
Abstract
Background: Congestion is a primary driver of symptoms in patients with acute heart failure, and relief of congestion is a critical goal of therapy. Monitoring of response to therapy through the assessment of daily weights and net fluid loss is the current standard of care, yet the relationship between commonly used markers of decongestion and both patient reported symptom relief and clinical outcomes are unknown.
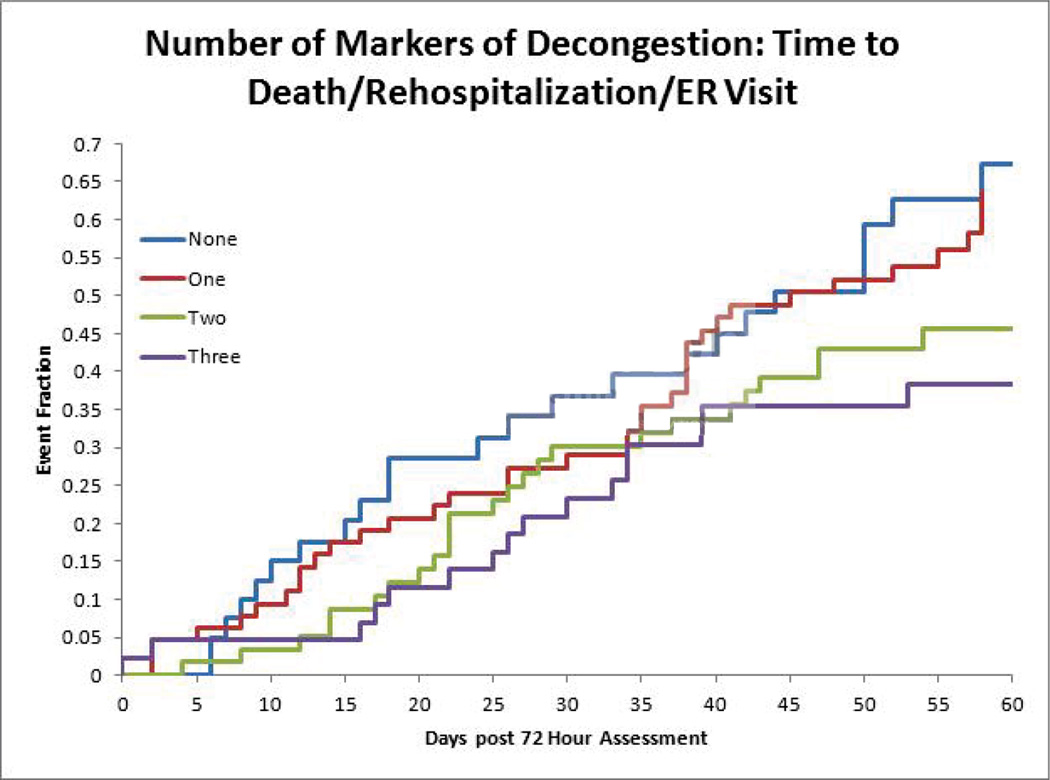
Methods and results: We performed a retrospective analysis of the randomized clinical trial, diuretic optimization strategy evaluation in acute heart failure (DOSE-AHF), enrolling patients hospitalized with a diagnosis of acute decompensated heart failure. We assessed the relationship among 3 markers of decongestion at 72 hours-weight loss, net fluid loss, and percent reduction in serum N terminal B-type natriuretic peptide (NT-proBNP) level-and relief of symptoms as defined by the dyspnea visual analog scale area under the curve. We also determined the relationship between each marker of decongestion and 60-day clinical outcomes defined as time to death, first rehospitalization or emergency department visit. Mean age was 66 years, mean ejection fraction was 35%, and 27% had ejection fraction ≥50%. Of the 3 measures of decongestion assessed, only percent reduction in NT-proBNP was significantly associated with symptom relief (r=0.13; P=0.04). There was no correlation between either weight loss or net fluid loss and symptom relief, (r=0.04; P=0.54 and r=0.07; P=0.27, respectively). Favorable changes in each of the 3 markers of decongestion were associated with improvement in time to death, rehospitalization, or emergency department visit at 60 days (weight: hazard ratio, 0.91; 95% confidence interval, 0.85-0.97 per 4 lbs; weight lost; fluid hazard ratio, 0.94; 95% confidence interval, 0.90-0.99 per 1000 mL fluid loss; NT-proBNP hazard ratio, 0.95; 95% confidence interval, 0.91-0.99 per 10% reduction). These associations were unchanged after multivariable adjustment with the exception that percent reduction in NT-proBNP was no longer a significant predictor (hazard ratio, 0.97; 95% confidence interval, 0.93-1.02). The rates of death, HF hospitalization, or emergency department visit at 60 days for patients with 0, 1, 2, and 3 markers of decongestion (above the median) were 67%, 64%, 46%, and 38%, respectively (log rank P value=0.05).
Conclusions: Weight loss, fluid loss, and NT-proBNP reduction at 72 hours are poorly correlated with dyspnea relief. However, favorable improvements in each of the 3 markers were associated with improved clinical outcomes at 60 days. These data suggest the need for ongoing research to understand the relationships among symptom relief, congestion, and outcomes in patients with acute decompensated heart failure.
Clinical trial registration: URL: http://www.clinicaltrials.gov. UNIQUE IDENTIFIER: NCT00577135.
Figures
References
-
- Adams KF, Jr, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, Berkowitz RL, Galvao M, Horton DP. Characteristics and outcomes of patients hospitalized for heart failure in the united states: Rationale, design, and preliminary observations from the first 100,000 cases in the acute decompensated heart failure national registry (adhere) Am Heart J. 2005;149:209–216. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update incorporated into the acc/aha 2005 guidelines for the diagnosis and management of heart failure in adults a report of the american college of cardiology foundation/american heart association task force on practice guidelines developed in collaboration with the international society for heart and lung transplantation. J Am Coll Cardiol. 2009;53:e1–e90. - PubMed
-
- West RL, Hernandez AF, O'Connor CM, Starling RC, Califf RM. A review of dyspnea in acute heart failure syndromes. Am Heart J. 2010;160:209–214. - PubMed
-
- Nohria A, Lewis E, Stevenson LW. Medical management of advanced heart failure. JAMA. 2002;287:628–640. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
