

Predictors of lithium response in bipolar disorder
- PMID: 23251751
- PMCID: PMC3513882
- DOI: 10.1177/2040622311399173
Predictors of lithium response in bipolar disorder
Abstract
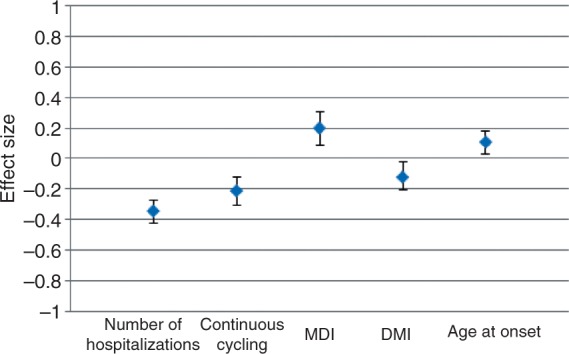
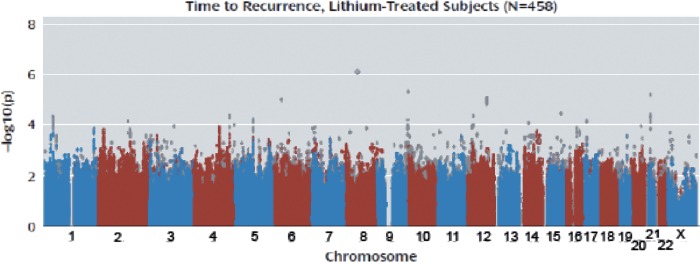
While lithium is generally regarded as the first-line agent for patients with bipolar disorder, it does not work for everyone, which raises the question: can we predict who will be most likely to respond? In this paper, we review the most compelling clinical, biologic, and genetic predictors of lithium response in bipolar disorder. Among clinical factors, the strongest predictors of good response are fewer hospitalizations preceding treatment, an episodic course characterized by an illness pattern of mania followed by depression, and a later age at onset of bipolar disorder. While several biologic predictors have been studied, the results are preliminary and require replication with studies of larger patient samples over longer observation periods. Neuroimaging is a particularly promising method given that it might concurrently illuminate pathophysiologic underpinnings of bipolar disorder, the mechanism of action of lithium, and potential predictors of lithium response. The first genome-wide association study of lithium response was recently completed. No definitive results emerged, perhaps because the study was underpowered. With major new initiatives in progress aiming to identify genes and genetic variations associated with lithium response, there is much reason to be hopeful that clinically useful information might be generated within the next several years. This could ultimately translate into tests that could guide the choice of mood-stabilizing medication for patients. In addition, it might facilitate pharmacologic research aimed at developing newer, more effective medications that might act more quickly and yield fewer side effects.
Keywords: bipolar disorder; genetics; lithium; neuroimaging; predicting response.
Conflict of interest statement
The authors have no conflicts of interest in preparing this article.
Figures
References
-
- Baastrup P.C., Poulsen J.C., Schou M., Thomsen K., Amdisen A. (1970) Prophylactic lithium: Double blind discontinuation in manic-depressive and recurrent-depressive disorders. Lancet 2: 326–330 - PubMed
-
- Baastrup P.C., Schou M. (1967) Lithium as a prophylactic agent. Its effect against recurrent depressions and manic-depressive psychosis. Arch Gen Psychiatry 16: 162–172 - PubMed
-
- Backlund L., Ehnvall A., Hetta J., Isacsson G., Agren H. (2009) Identifying predictors for good lithium response - a retrospective analysis of 100 patients with bipolar disorder using a life-charting method. Eur Psychiatry 24: 171–177 - PubMed
-
- Berghofer A., Alda M., Adli M., Baethge C., Bauer M., Bschor T., et al. (2008) Long-term effectiveness of lithium in bipolar disorder: A multicenter investigation of patients with typical and atypical features. J Clin Psychiatry 69: 1860–1868 - PubMed
-
- Bremer T., Diamond C., McKinney R., Shehktman T., Barrett T.B., Herold C., et al. (2007) The pharmacogenetics of lithium response depends upon clinical co-morbidity. Mol Diag Ther 11: 161–170 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
