

The impact of immediate reporting on interpretive discrepancies and patient referral pathways within the emergency department: a randomised controlled trial
- PMID: 23255536
- PMCID: PMC3615405
- DOI: 10.1259/bjr.20120112
The impact of immediate reporting on interpretive discrepancies and patient referral pathways within the emergency department: a randomised controlled trial
Abstract
Objective: To determine whether an immediate reporting service for musculoskeletal trauma reduces interpretation errors and positively impacts on patient referral pathways.
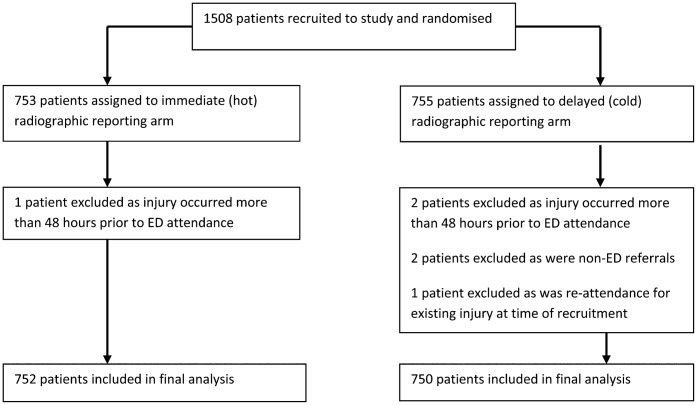
Methods: A pragmatic multicentre randomised controlled trial was undertaken. 1502 patients were recruited and randomly assigned to an immediate or delayed reporting arm and treated according to group assignment. Assessment was made of concordance in image interpretation between emergency department (ED) clinicians and radiology; discharge and referral pathways; and patient journey times.
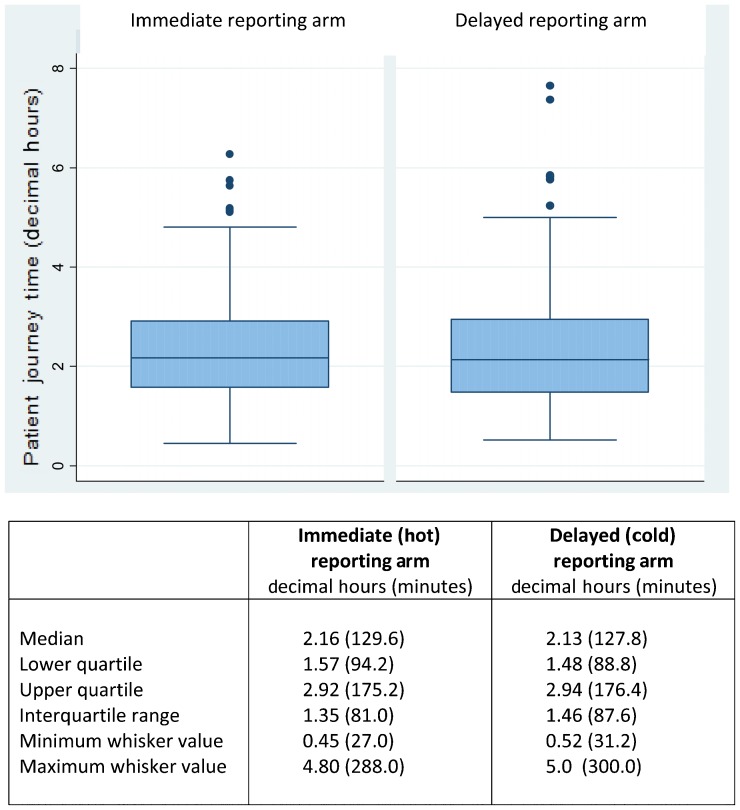
Results: 1688 radiographic examinations were performed (1502 patients). 91 discordant interpretations were identified (n=91/1688; 5.4%) with a greater number of discordant interpretations noted in the delayed reporting arm (n=67/849, 7.9%). In the immediate reporting arm, the availability of a report reduced, but did not eliminate, discordance in interpretation (n=24/839, 2.9%). No significant difference in number of patients discharged, referred to hospital clinics or admitted was identified. However, patient ED recalls were significantly reduced (z=2.66; p=0.008) in the immediate reporting arm, as were the number of short-term inpatient bed days (5 days or less) (z=3.636; p<0.001). Patient journey time from ED arrival to discharge or admission was equivalent (z=0.79, p=0.432).
Conclusion: Immediate reporting significantly reduced ED interpretive errors and prevented errors that would require patient recall. However, immediate reporting did not eliminate ED interpretative errors or change the number of patients discharged, referred to hospital clinics or admitted overall.
Advances in knowledge: This is the first study to consider the wider impact of immediate reporting on the ED patient pathway as a whole and hospital resource usage.
Figures
References
-
- Department of Health. A&E attendances. [cited 20 September 2011]. Available from: http://www.dh.gov.uk/en/Publicationsandstatistics/Statistics/Performance....
-
- NHS Information Centre. Accident and emergency attendances in England (experimental statistics) 2009–10. [cited 23 September 2011]. Available from: http://www.ic.nhs.uk/statistics-and-data-collections/hospital-care/accid....
-
- de Lacey G. Number of casualty attenders referred for X-ray examination. Br J Radiol 1979;52:52–3. - PubMed
-
- Richards PJ, Tins B, Cherian R, Rae F, Dharmarajah R, Phair IC, et al. The emergency department: an appropriate referral rate for radiography. Clin Radiol 2002;57:753–8. - PubMed
-
- Nolan TM, Oberklaid F, Boldt D. Radiological services in a hospital emergency department—an evaluation of service delivery and radiograph interpretation. Aust Paediatr J 1984;20:109–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
