

Review
doi: 10.1152/ajpcell.00328.2012.
Epub 2012 Dec 19.
Cellular mechanisms of tissue fibrosis. 1. Common and organ-specific mechanisms associated with tissue fibrosis
Affiliations
- PMID: 23255577
- PMCID: PMC3566435
- DOI: 10.1152/ajpcell.00328.2012
Item in Clipboard
Review
Cellular mechanisms of tissue fibrosis. 1. Common and organ-specific mechanisms associated with tissue fibrosis
Am J Physiol Cell Physiol.
.
Abstract
Fibrosis is a pathological scarring process that leads to destruction of organ architecture and impairment of organ function. Chronic loss of organ function in most organs, including bone marrow, heart, intestine, kidney, liver, lung, and skin, is associated with fibrosis, contributing to an estimated one third of natural deaths worldwide. Effective therapies to prevent or to even reverse existing fibrotic lesions are not yet available in any organ. There is hope that an understanding of common fibrosis pathways will lead to development of antifibrotic therapies that are effective in all of these tissues in the future. Here we review common and organ-specific pathways of tissue fibrosis.
Figures
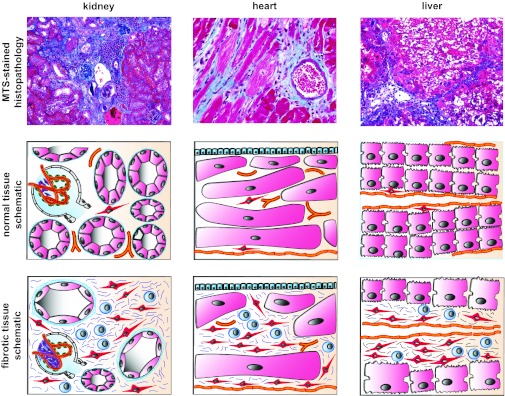
Common features of tissue fibrosis. Macroscopically and microscopically fibrotic organs share obvious commonalities, which has led to the concept of common fibrotic pathways: fibrotic organs are stiff [reflecting excessive extracellular matrix (ECM) deposition], are pale (reflecting rarefication of the vasculature), and have an uneven surface (reflecting fibroblast contraction). Histopathological analysis reveals that tissue fibrosis is unequivocally associated with injury of the parenchyme, accumulation of fibrillar ECM, accumulation of fibroblasts, rarefication of the microvasculature, and a mononuclear infiltrate. The figure illustrates the common appearance of fibrotic kidney, heart, and liver. The photomicrographs display representative MTS-stained sections of fibrotic mouse kidney, heart, and lung. Schematics illustrate the common mechanisms of tissue fibrosis: each organ consists of a functional parenchyme (pink, tubular epithelium in kidney, cardiomyocytes in heart, and hepatocytes in liver) and a connective tissue compartment containing microvessels (orange) and fibroblasts (red, and stellate cells in the liver). Fibrosis is unequivocally associated with expansion of the connective tissue compartment. The fibrotic connective tissue contains ECM fibers (blue), activated fibroblasts (red), and a mononuclear infiltrate (blue). The question is whether common or organ-specific mechanisms lead to this uniform appearance.
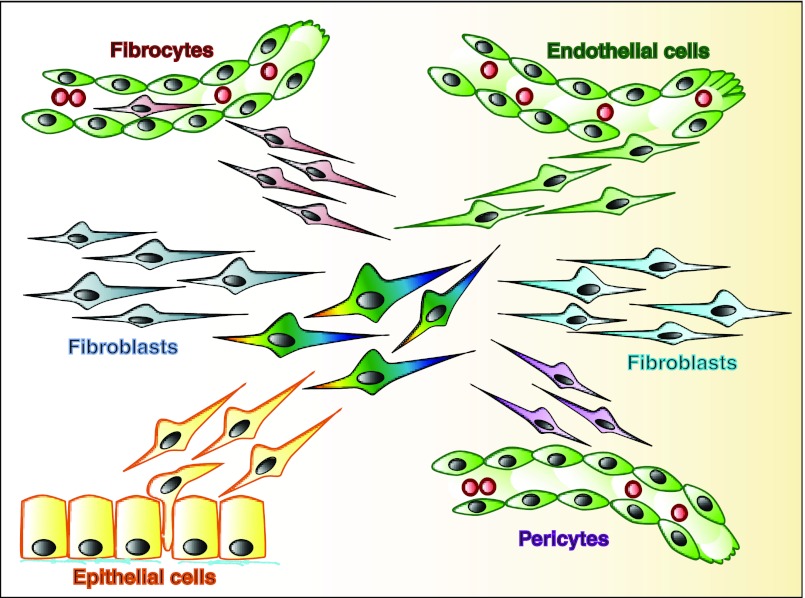
Origins of activated fibroblasts. Fibrosis is associated with accumulation of collagen-producing (activated) fibroblasts (center, multicolored). Activated fibroblasts can derive via activation and subsequent proliferation from resident fibroblasts (blue). Bone marrow-derived fibrocytes are recruited to fibrotic lesions and contribute to accumulation of collagen-producing fibroblasts (red, top left). Endothelial cells can undergo an endothelial-to-mesenchymal transition to contribute to fibroblast accumulation (green, top right). α-Smooth muscle actin (αSMA)-positive vascular smooth muscle cells and pericytes have been proposed to shed off existing vessels and to contribute to accumulation of myofibroblasts (pink, bottom right). Epithelial cells can undergo an epithelial-to-mesenchymal transition and contribute to fibroblast accumulation (yellow, bottom left).
References
-
- Abraham DJ, Shiwen X, Black CM, Sa S, Xu Y, Leask A. Tumor necrosis factor alpha suppresses the induction of connective tissue growth factor by transforming growth factor-beta in normal and scleroderma fibroblasts. J Biol Chem 275: 15220–15225, 2000 - PubMed
-
- Abraham DJ, Varga J. Scleroderma: from cell and molecular mechanisms to disease models. Trends Immunol 26: 587–595, 2005 - PubMed
-
- Akram KM, Lomas NJ, Spiteri MA, Forsyth NR. Clara cells inhibit alveolar epithelial wound repair via TRAIL-dependent apoptosis. Eur Respir J. Epub ahead of print doi:10.1183/09031936.00213411 - DOI - PubMed
-
- Akram KM, Samad S, Spiteri M, Forsyth NR. Mesenchymal stem cell therapy and lung diseases. Adv Biochem Eng Biotechnol. Epub ahead of print doi:10.1007/10_2012_140 - DOI - PubMed
-
- Anders HJ, Muruve DA. The inflammasomes in kidney disease. J Am Soc Nephrol 22: 1007–1018, 2011 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical