

Lung Ultrasound in the Critically Ill Neonate
- PMID: 23255876
- PMCID: PMC3522086
- DOI: 10.2174/157339612802139389
Lung Ultrasound in the Critically Ill Neonate
Abstract
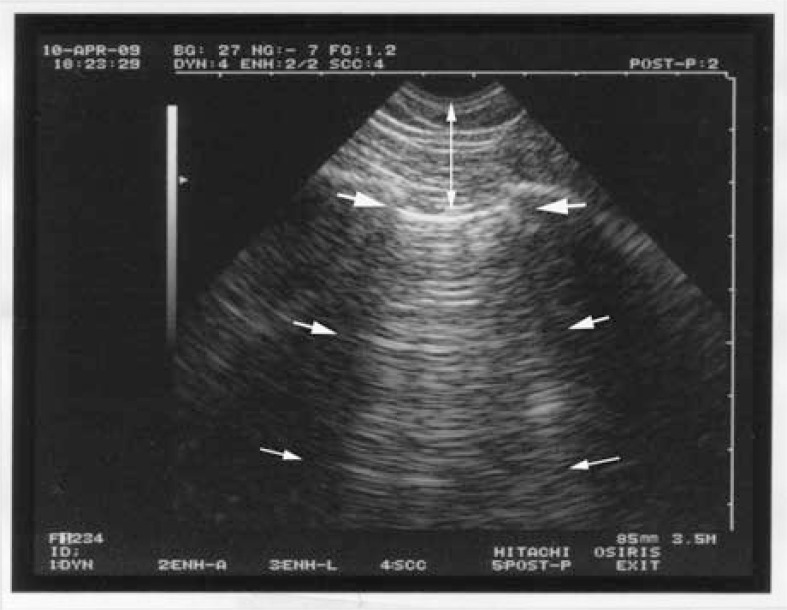
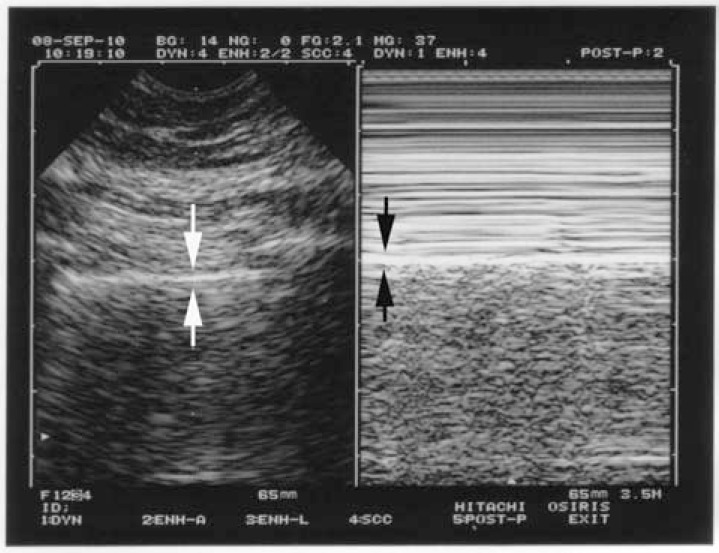
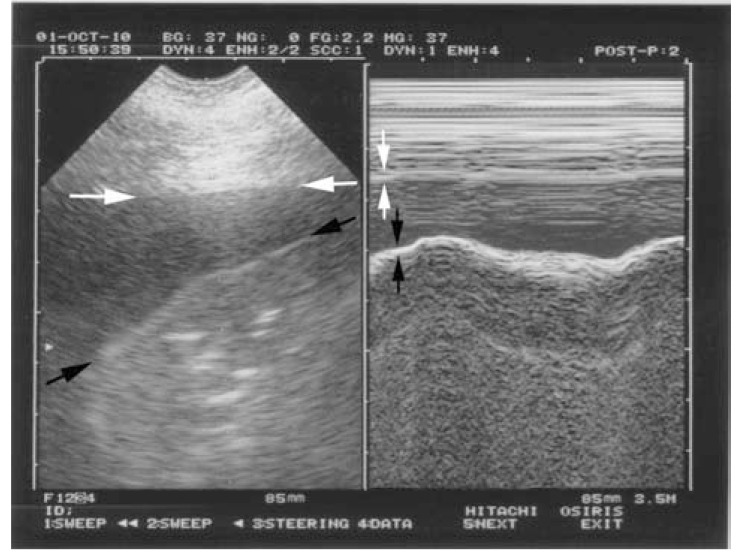
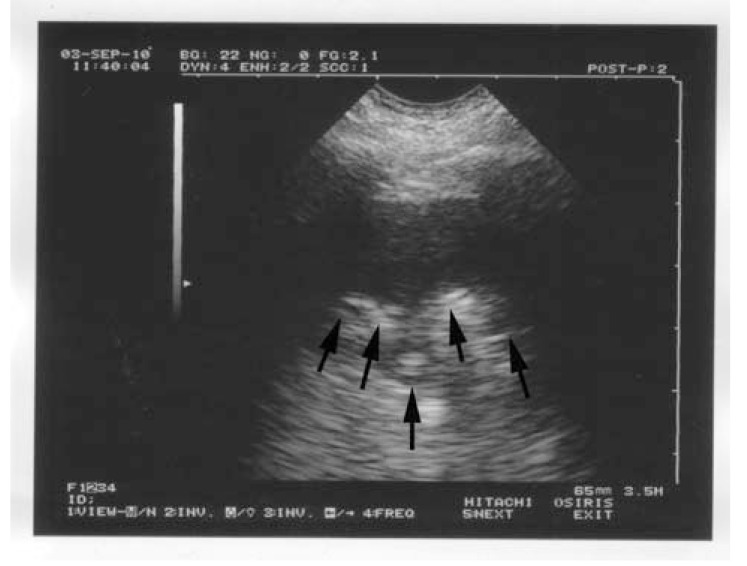
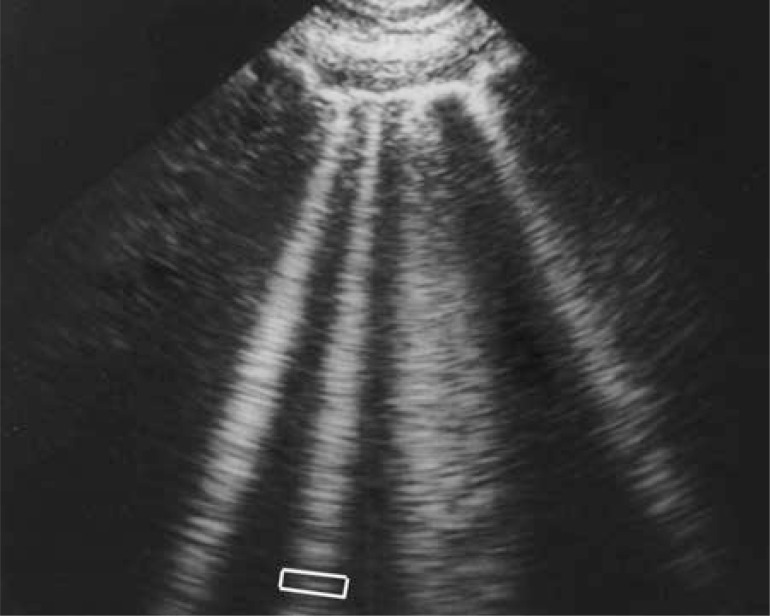
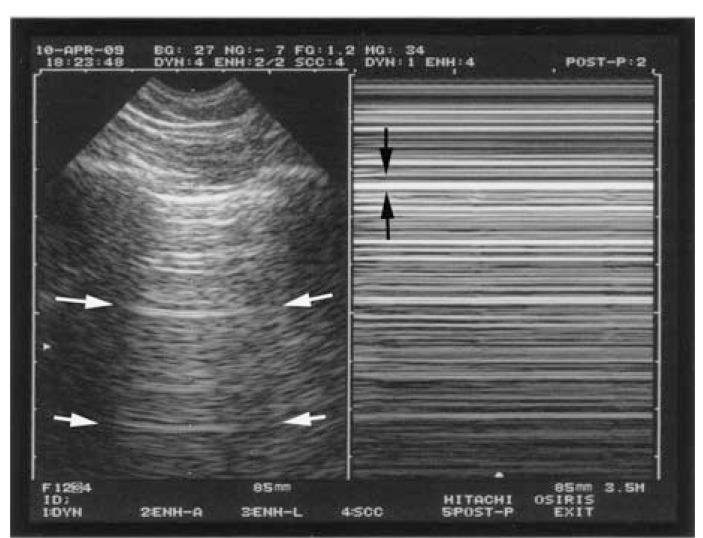
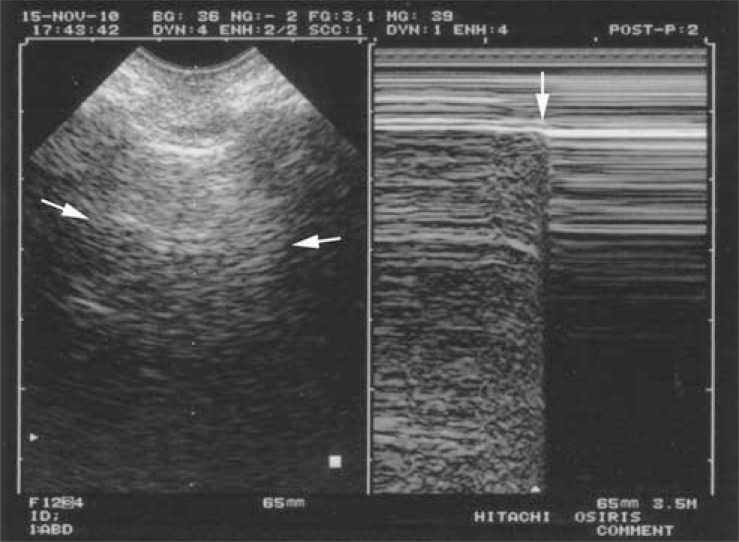
Critical ultrasound is a new tool for first-line physicians, including neonate intensivists. The consideration of the lung as one major target allows to redefine the priorities. Simple machines work better than up-to-date ones. We use a microconvex probe. Ten standardized signs allow a majority of uses: the bat sign (pleural line), lung sliding and the A-line (normal lung surface), the quad sign and sinusoid sign indicating pleural effusion regardless its echogenicity, the tissue-like sign and fractal sign indicating lung consolidation, the B-line artifact and lung rockets (indicating interstitial syndrome), abolished lung sliding with the stratosphere sign, suggesting pneumothorax, and the lung point, indicating pneumothorax. Other signs are used for more sophisticated applications (distinguishing atelectasis from pneumonia for instance...). All these disorders were assessed in the adult using CT as gold standard with sensitivity and specificity ranging from 90 to 100%, allowing to consider ultrasound as a reasonable bedside gold standard in the critically ill. The same signs are found, with no difference in the critically ill neonate. Fast protocols such as the BLUE-protocol are available, allowing immediate diagnosis of acute respiratory failure using seven standardized profiles. Pulmonary edema e.g. yields anterior lung rockets associated with lung sliding, making the B-profile. The FALLS-protocol, inserted in a Limited Investigation including a simple model of heart and vessels, assesses acute circulatory failure using lung artifacts. Interventional ultrasound (mainly, thoracocenthesis) provides maximal safety. Referrals to CT can be postponed. CEURF proposes personnalized bedside trainings since 1990. Lung ultrasound opens physicians to a visual medicine.
Figures

References
-
- Dénier A. Les ultrasons, leur application au diagnostic. Presse Méd. 1946;22:307–8.
-
- Greenough A, Dimitriou G, Alvares BR, Karani J. Routine daily chest radiographs in ventilated, very low birth weight infants. Eur J Pediatr. 2001;160:147–9. - PubMed
-
- Spitzer AR, Greer JG, Antunes M, Szema KF, Gross GW. The clinical value of screening chest radiography in the neonate with lung disease. Clin Pediatr. 1993;32:514–9. - PubMed
-
- Hauser GJ, Pollack MM, Sivit CJ, Taylor GA, Bulas DI, Guion CJ. Routine chest radiographs in pediatric intensive care: a prospective study. Pediatrics. 1989;83:465–70. - PubMed
-
- Weinberger SE, Drazen JM. Harrison’s principles of internal medicine. Ed. 16. New York: McGraw-Hill; 2005. Diagnostic procedures in respiratory diseases; pp. 1505–8.
LinkOut - more resources
Full Text Sources