

Analysis of complete response by MRI following neoadjuvant chemotherapy predicts pathological tumor responses differently for molecular subtypes of breast cancer
- PMID: 23255899
- PMCID: PMC3525359
- DOI: 10.3892/ol.2012.1004
Analysis of complete response by MRI following neoadjuvant chemotherapy predicts pathological tumor responses differently for molecular subtypes of breast cancer
Erratum in
-
Corrigendum.Oncol Lett. 2013 Apr;5(4):1433. doi: 10.3892/ol.2013.1141. Oncol Lett. 2013. PMID: 23599809 Free PMC article.
Abstract
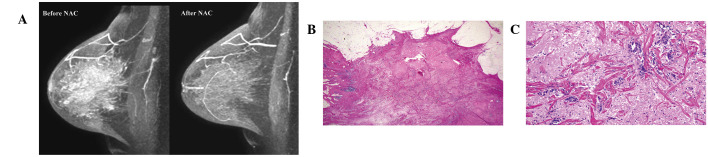
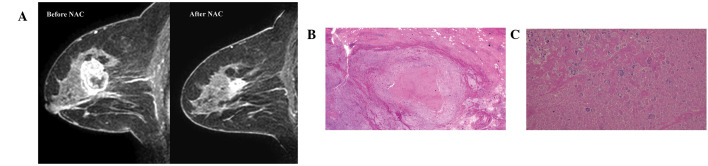
In the present study, clinical tumor response following neoadjuvant chemotherapy (NAC) was diagnosed by magnetic resonance imaging (MRI) and clinicopathological factors, including molecular subtypes at baseline, were analyzed for correlations with pathological tumor responses. In addition, clinicopathological factors were analyzed for a correlation with the MRI capacity to predict pathological complete response (pCR). Clinical tumor response evaluated by MRI following NAC was determined as a clinical CR (cCR) or a residual tumor. cCR was confirmed if no gadolinium enhancement or an enhancement equal to or less than that of glandular tissue was observed in any phase of the MRI. Pathological tumor responses following NAC were classified into grades 0 (no change) to 3 (no residual invasive cancer) according to criteria of the Japanese Breast Cancer Society. pCR was defined as grade 3 in the present study. Of 264 cases of invasive breast cancer in 260 patients (4 synchronous bilateral breast cancer cases), 59 (22%) were diagnosed by MRI following NAC as cCR and 98 (37%) were pathologically diagnosed as pCR. In terms of predicting pCR by MRI, the sensitivity, specificity, accuracy, positive predictive value (PPV) and negative predictive value (NPV) were 44, 90, 73, 73 and 73%, respectively. Tumor size, hormone receptor status, human epidermal growth factor receptor 2 (HER2) status, molecular subtype and histological type were significantly correlated with pathological tumor responses. pCR rates increased in the following order: luminal/HER2-negative (14%), luminal/HER2-positive (32%), triple-negative (46%) and non-luminal/HER2-positive (73%) tumors. Sensitivity and specificity were the highest (60 and 100%, respectively) in triple-negative tumors. PPV decreased in the following order: triple-negative (100%), non-luminal/HER2-positive (92%), luminal/HER2-positive (46%) and luminal/HER2-negative (33%) tumors. In conclusion, MRI evaluation is useful for predicting pCR following NAC, particularly for triple-negative tumors.
Figures
References
-
- Fisher B, Bryant J, Wolmark N, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol. 1998;16:2672–2685. - PubMed
-
- Rastogi P, anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol. 2008;26:778–785. - PubMed
-
- Symmans WF, Peintinger F, Hatzis C, et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J Clin Oncol. 2007;25:4414–4422. - PubMed
-
- Smith IC, Heys SD, Hutcheon AW, et al. Neoadjuvant chemotherapy in breast cancer: significantly enhanced response with docetaxel. J Clin Oncol. 2002;20:1456–1466. - PubMed
-
- Buzdar AU, Valero V, Ibrahim NK, et al. Neoadjuvant therapy with paclitaxel followed by 5-fluorouracil, epirubicin and cyclophosphamide chemotherapy and concurrent trastuzumab in human epidermal growth factor receptor 2-positive operable breast cancer: an update of the initial randomized study population and data of additional patients treated with the same regimen. Clin Cancer Res. 2007;13:228–233. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous