

Hypothyroidism and mortality among dialysis patients
- PMID: 23258793
- PMCID: PMC3613957
- DOI: 10.2215/CJN.06920712
Hypothyroidism and mortality among dialysis patients
Abstract
Background and objectives: Hypothyroidism is highly prevalent among ESRD patients, but its clinical significance and the benefits of thyroid hormone replacement in this context remain unclear.
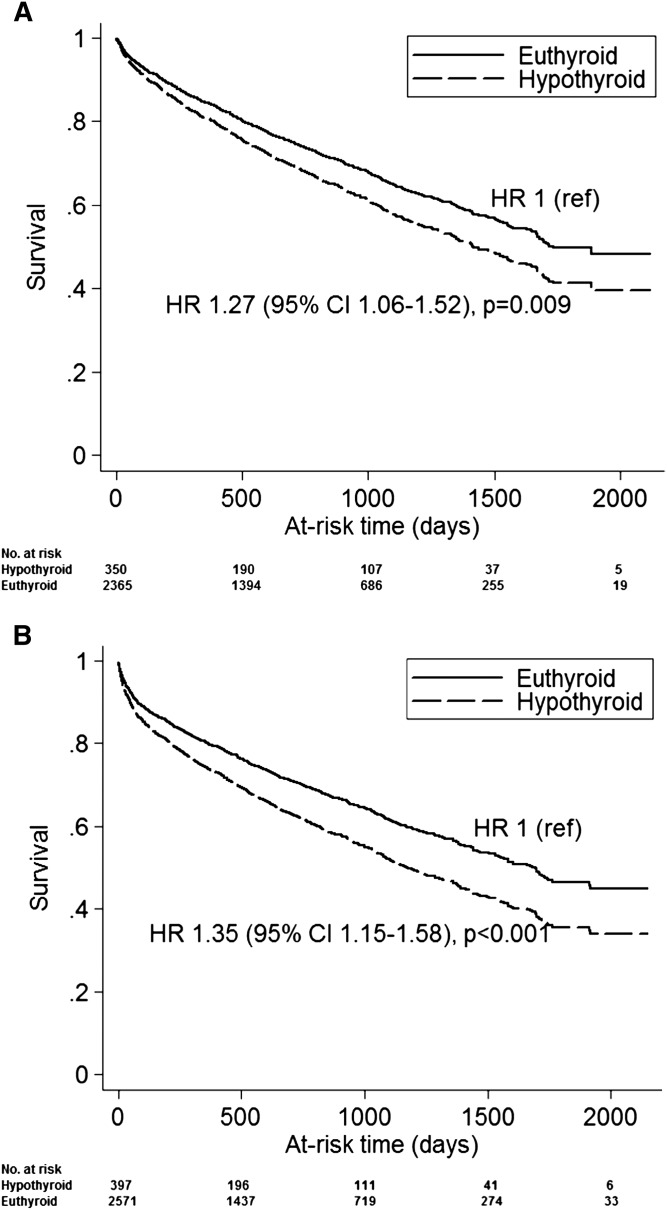
Design, setting, participants, & measurements: This study examined the association between hypothyroidism and all-cause mortality among 2715 adult dialysis patients with baseline thyrotropin levels measured between April of 2005 and April of 2011. Mortality was ascertained from Social Security Death Master Index and local registration systems. The association between hypothyroidism (thyrotropin greater than assay upper limit normal) and mortality was estimated using Cox proportional hazards models. To reduce the risk of observing reverse-causal associations, models included a 30-day lag between thyrotropin measurement and at-risk time.
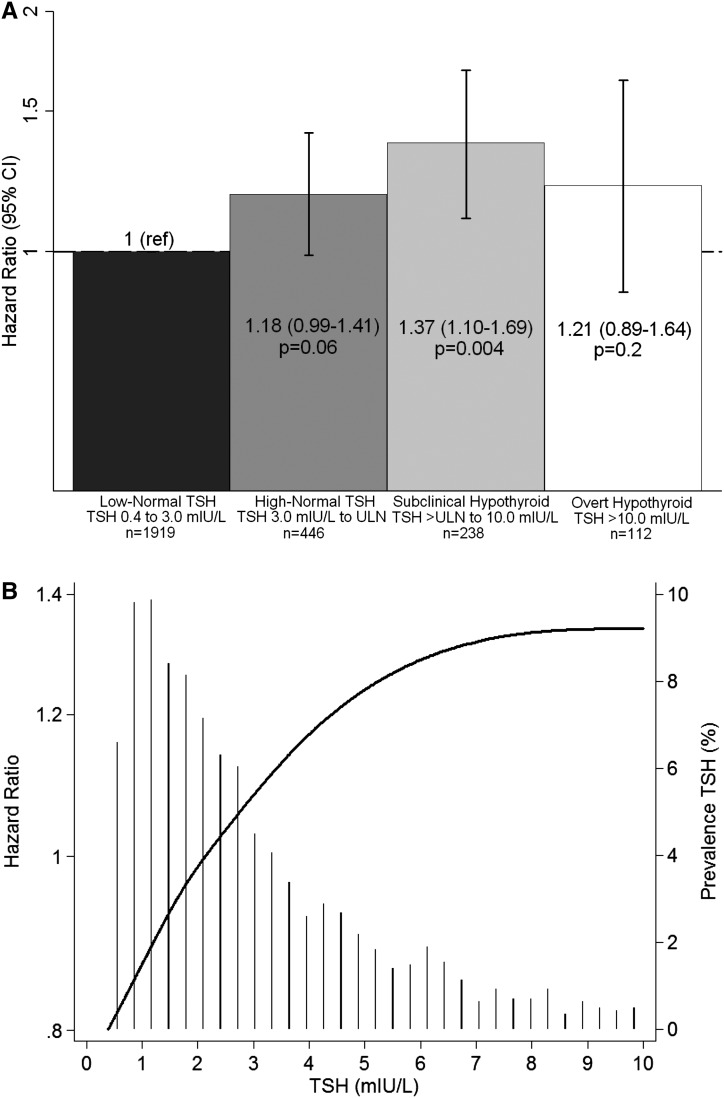
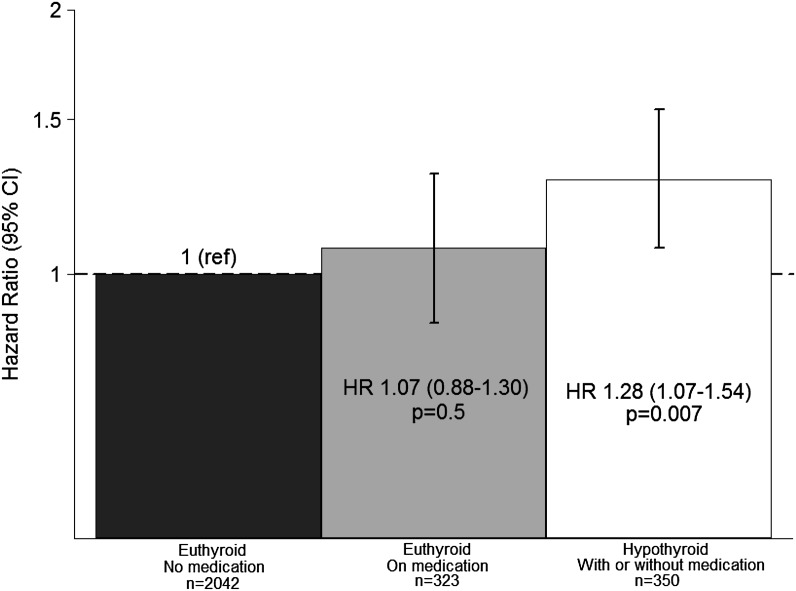
Results: Among 350 (12.9%) hypothyroid and 2365 (87.1%) euthyroid (assay within referent range) patients, 917 deaths were observed during 5352 patient-years of at-risk time. Hypothyroidism was associated with higher mortality. Compared with thyrotropin in the low-normal range (0.4-2.9 mIU/L), subclinical hypothyroidism (thyrotropin >upper limit normal and ≤10.0 mIU/L) was associated with higher mortality; high-normal thyrotropin (≥3.0 mIU/L and ≤upper limit normal) and overt hypothyroidism (thyrotropin >10.0 mIU/L) were associated with numerically greater risk, but estimates were not statistically significant. Compared with spontaneously euthyroid controls, patients who were euthyroid while on exogenous thyroid replacement were not at higher mortality risk, whereas patients who were hypothyroid were at higher mortality risk. Sensitivity analyses indicated that effects on cardiovascular risk factors may mediate the observed association between hypothyroidism and death.
Conclusions: These data suggest that hypothyroidism is associated with higher mortality in dialysis patients, which may be ameliorated by thyroid hormone replacement therapy.
Figures
References
-
- Kaptein EM: Thyroid hormone metabolism and thyroid diseases in chronic renal failure. Endocr Rev 17: 45–63, 1996 - PubMed
-
- Kaptein EM, Quion-Verde H, Chooljian CJ, Tang WW, Friedman PE, Rodriquez HJ, Massry SG: The thyroid in end-stage renal disease. Medicine (Baltimore) 67: 187–197, 1988 - PubMed
-
- Lo JC, Chertow GM, Go AS, Hsu CY: Increased prevalence of subclinical and clinical hypothyroidism in persons with chronic kidney disease. Kidney Int 67: 1047–1052, 2005 - PubMed
