

Risk factors for graft loss and mortality after renal transplantation according to recipient age: a prospective multicentre study
- PMID: 23258810
- PMCID: PMC3526982
- DOI: 10.1093/ndt/gfs544
Risk factors for graft loss and mortality after renal transplantation according to recipient age: a prospective multicentre study
Abstract
Background: To describe the causes of graft loss, patient death and survival figures in kidney transplant patients in Spain based on the recipient's age.
Methods: The results at 5 years of post-transplant cardiovascular disease (CVD) patients, taken from a database on CVD, were prospectively analysed, i.e. a total of 2600 transplanted patients during 2000-2002 in 14 Spanish renal transplant units, most of them receiving their organ from cadaver donors. Patients were grouped according to the recipient's age: Group A: <40 years, Group B: 40-60 years and Group C: >60 years. The most frequent immunosuppressive regimen included tacrolimus, mycophenolate mofetil and steroids.
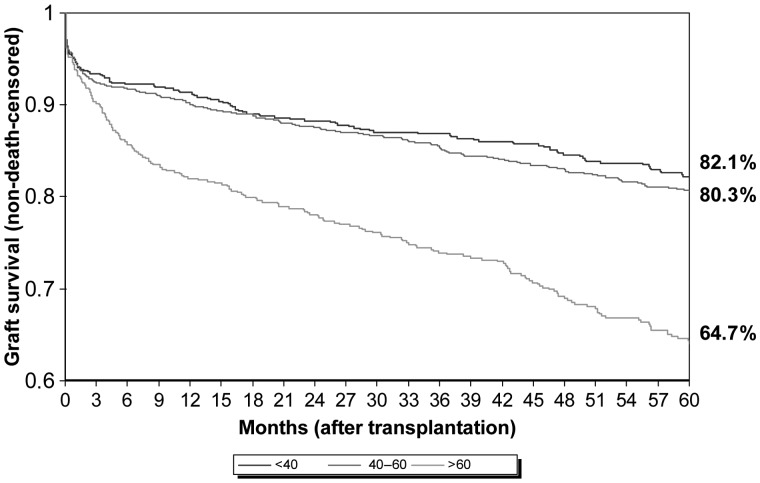
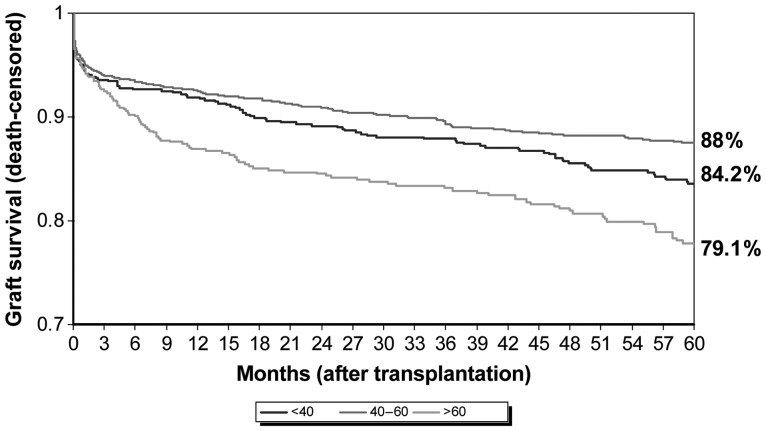
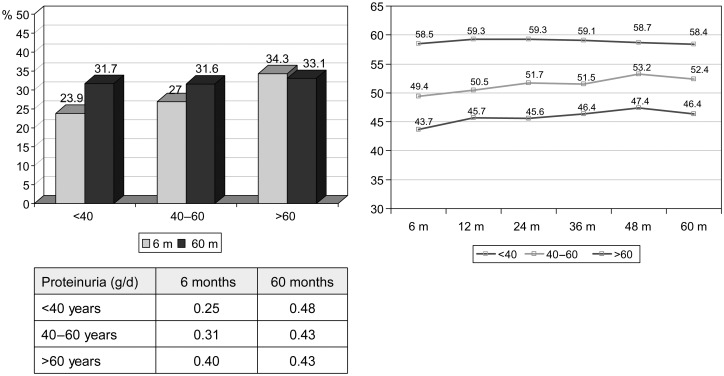
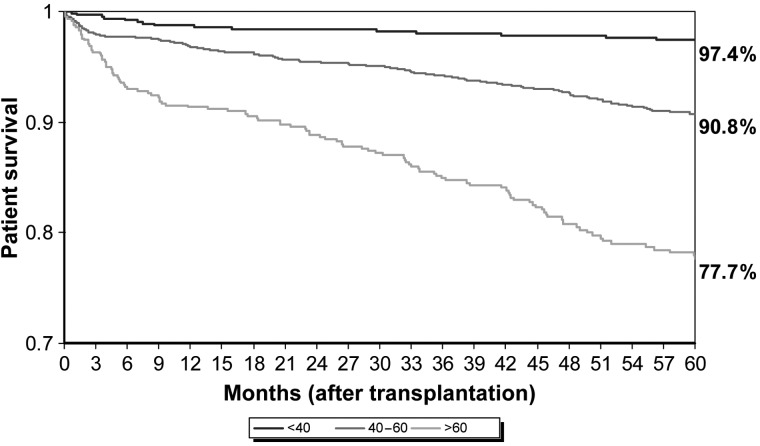
Results: Patients were distributed as follows: 25.85% in Group A (>40 years), 50.9% in Group B (40-60 years) and 23.19% in Group C (>60). The 5-year survival for the different age groups was 97.4, 90.8 and 77.7%, respectively. Death-censored graft survival was 88, 84.2 and 79.1%, respectively, and non death-censored graft survival was 82.1, 80.3 and 64.7%, respectively. Across all age groups, CVD and infections were the most frequent cause of death. The main causes of graft loss were chronic allograft dysfunction in patients <40 years old and death with functioning graft in the two remaining groups. In the multivariate analysis for graft survival, only elevated creatinine levels and proteinuria >1 g at 6 months post-transplantation were statistically significant in the three age groups. The patient survival multivariate analysis did not achieve a statistically significant common factor in the three age groups.
Conclusions: Five-year results show an excellent recipient survival and graft survival, especially in the youngest age group. Death with functioning graft is the leading cause of graft loss in patients >40 years. Early improvement of renal function and proteinuria together with strict control of cardiovascular risk factors are mandatory.
Figures
References
-
- Pascual M, Theruvath T, Kawai T, et al. Strategies to improve long-term outcomes after renal transplantation. N Engl J Med. 2002;346:580. - PubMed
-
- Woodroffe R, Yao GL, Meads C, et al. Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation. A systematic review and modelling study. Health Technol Assess. 2005;9:1. - PubMed
-
- Hariharan S, Johnson CP, Bresnahan BA, et al. Improved graft survival after renal transplantation in the United States, 1998 to 1996. N Engl J Med. 2000;342:605. - PubMed
-
- Meier-Kriesche HU, Schold JD, Srinivas TR, et al. Lack of improvement in renal allograft survival despite a marked decrease of acute rejection rates over the most recent era. Am J Transplant. 2004;4:378. - PubMed
-
- Foley RN, Parfrey PS, Samak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(Suppl 3):112–119. - PubMed
